Loading...

Foramen transversarium fracture (EDNeurorad Case 24)
149 views8 months agoThere is a minimally displaced fracture of the right transverse process of C6 extending to the foramen transversarium (@Key Finding 1). The fracture line also extends to the pedicle (@Key Finding 2). When fracture lines involve the foramen transversarium, a CTA commonly follows to assess for injury to the vertebral artery.
Cervical spineCT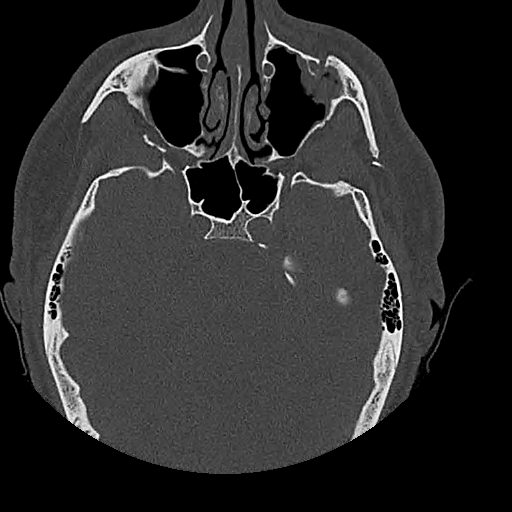
Zygomatico-maxillary complex fracture (EDNeurorad Case 23)
140 views8 months agoAll components of a left sided Zygomatico-maxillary complex (ZMC) fracture are present (aka tetrapod fracture): Fracture of the lateral left maxillary sinus at the level of the zygomatico-maxillary suture (@Key Finding 1), segmental fracture of the left zygomatic arch extending to the zygomatico-temporal suture (@Key Finding 2), fracture of the left zygomatico-sphenoid suture (@Key Finding 3), and fracture/diasthasis of the left zygomatico-frontal suture (@Key Finding 4).
HeadCT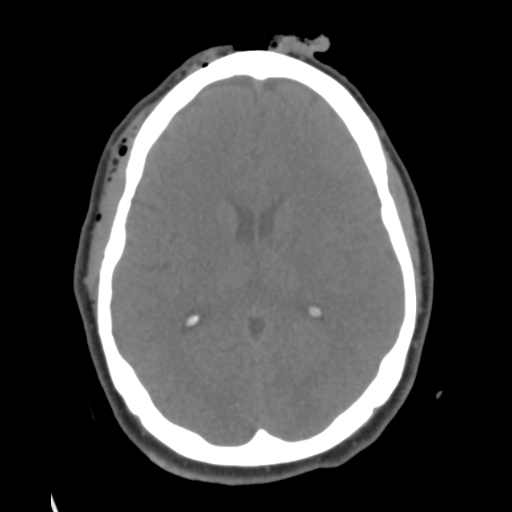
Left atlanto-occipital injury (EDNeurorad Case 22)
136 views8 months agoThere is a mildly displaced fracture of the left occipital condyle (@Key Finding 1 and @Key Finding 3). In addition, there is a mildly displaced fracture of the left lateral mass of C1 (@Key Finding 2). Cervical spine CT might not always be obtained at the same time as the head CT so include the craniocervical junction in your head CT search pattern.There is also extensive soft tissue laceration to the right forehead (@Key Finding 4) with an associated minimally displaced fracture of the right superolateral orbital rim (@Key Finding 5).
HeadCT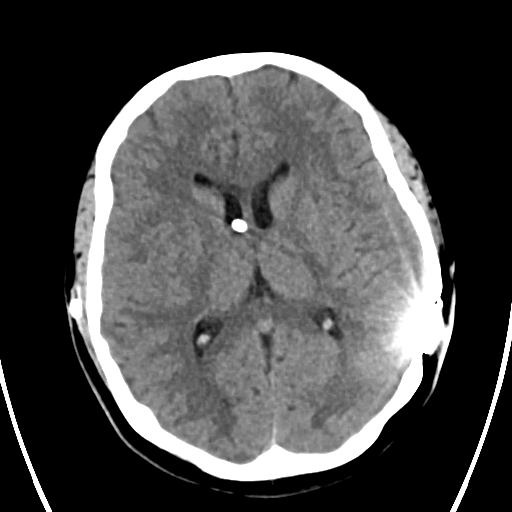
VP shunt catheter break (EDNeurorad Case 21)
136 views8 months agoWhile the ventricular system is not enlarged, there is a break in the ventriculoperitoneal shunt catheter tubing inferior to reservoir, confirmed on subsequent revision (@Key Finding 1). The two ends of the broken catheter are shown in the MIP key finding image but should of course be confirmed broken by reviewing the source images as well. Always include assessment of the shunt tubing integrity part of your search pattern.
HeadCT
Mandibular fractures (EDNeurorad Case 20)
118 views8 months agoMax-face CT redemonstrates the displaced left mandibular fracture at the junction of the ramus and condylar process (@Key Finding 1). There is an additional minimally displaced right parasymphyseal fracture as well, "completing the ring." (@Key Finding 2)
HeadCT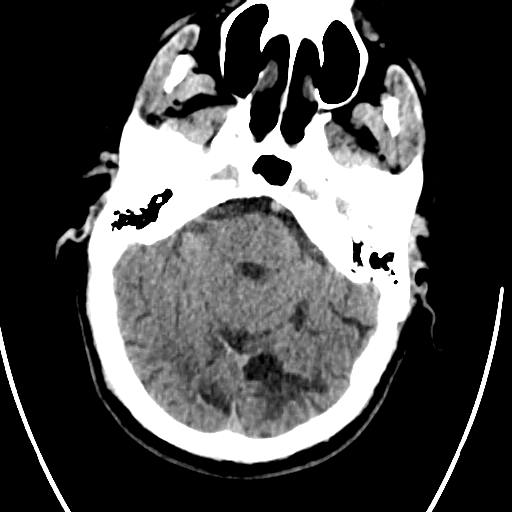
Left mandibular fracture (EDNeurorad Case 19)
115 views8 months agoThe major traumatic finding here is that there is a mildly displaced, mildly angulated fracture of the left mandibular ramus at the junction with the coronoid process (@Key Finding 1). Mandibular fractures frequently "complete the ring" so we need to get whole mandible imaging to look for a second fracture given that there is no TMJ dislocation.
HeadCT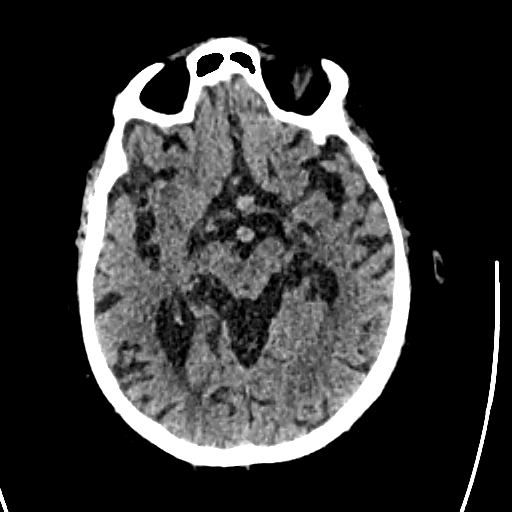
Anterior communicating aneurysm (EDNeurorad Case 18a)
139 views8 months agoThe most notable finding here is the incidental strong evidence for an anterior communicating aneurysm (@Key Finding 1, @Key Finding 2). With enough brain volume loss and with high enough resolution head CT, there is enough contrast between the arteries and the expanded CSF spaces for small aneurysms to become visible even on non-con CT.The patient does have a small right parietal scalp hematoma.
HeadCT
Intracranial hypotension (EDNeurorad Case 17)
136 views8 months agoIn addition to the morphologic features of intracranial hypotension described in the precursor case (@Key Finding 1), MRI also shows characteristic diffuse pachymeningeal enhancement (@Key Finding 2). On MRI, you can also more accurately observe the ponto-mamillary distance to be small, another feature of intracranial hypotension.See: Intracranial Hypotension: Improved MRI Detection With Diagnostic Intracranial Angles
BrainMRI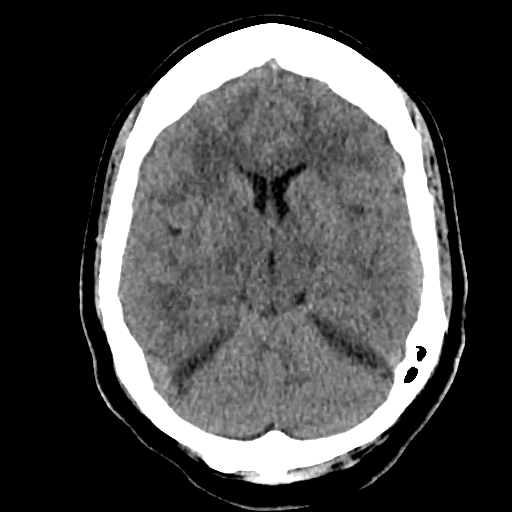
Intracranial hypotension (EDNeurorad Case 16)
159 views8 months agoThere are bilateral low attenuation upper cerebellar convexity subdural collections (@Key Finding 1). The attenuation is slightly greater than CSF so most likely they would be chronic subdural hematomas and less likely subdural hygromas.On the axial images, near complete effacement of the prepontine cistern (shown in @Key Finding 2 as the pons flush against the clivus) can be observed. The collections above are too small to be causing this much mass effect. Looking at sagital reformations (@Key Finding 3), we can see prominent appearance of the pituitary gland, a "sagging" appearance to the brain which abuts the pituitary, as well as sagging brainstem and mild cerebellar tonsillar ectopia. These findings, in addition to the bilateral subdural collections, are quite characteristic of intracranial hypotension.
HeadCT
