Loading...
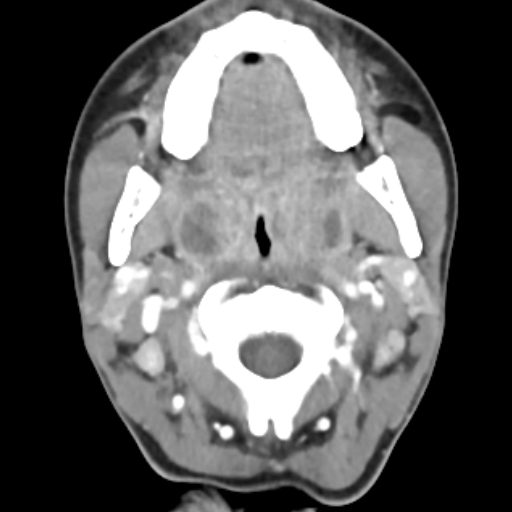
Submandibular sialadenitis due to sialolithiasis (EDNeurorad Case 34)
116 views8 months agoDue to underlying Sjogren's syndrome, there is extreme fatty replacement of both submandibular (shown on @Key Finding 1) and the parotid glands. However, the right submandibular gland is enlarged compared to the left, has internal edema and increased attenuation, substantial surrounding stranding as well as infiltrative edema extending to the adjacent tissues. Notice how on @Key Finding 1, the edema extends to the right aspect of the oropharynx and results in effacement of the right vallecula compared to the left (green arrow).On @Key Finding 2, you can see bilateral distal submandibular duct stones. There are quite a few more stones (@Key Finding 3, @Key Finding 4). The right submandibular duct is dilated (@Key Finding 4 and @Key Finding 5) and has mucosal hyperenhancement (@Key Finding 5).These constellation of finding are consistent with right submandibular sialadenitis due to sialolithiasis.
NeckCT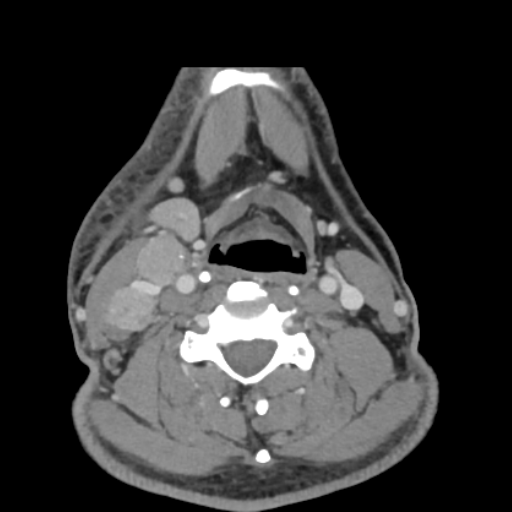
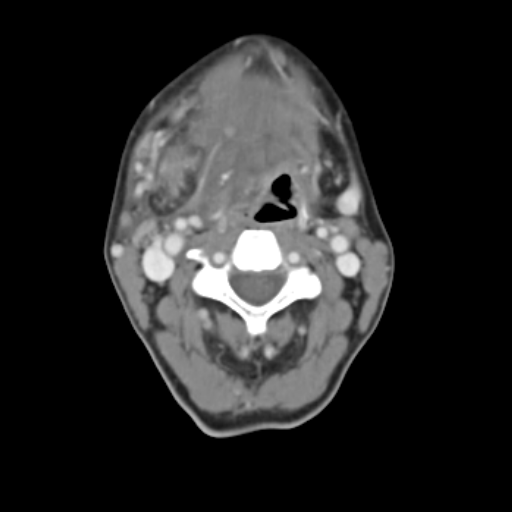
Right face cellulitis, metastatic papillary thyroid cancer, pulmonary adenocarcinoma (EDNeurorad Case 33)
130 views8 months ago@Key Finding 1 demonstrated right facial cutaneous thickening (white arrow) with subcutaneous stranding and thickening of the platysma muscle (red arrow) which are suggestive of underlying cellulitis. The source of the infection is not clear. There is clearly lymphadenopathy in the right neck. While in the setting of cellulitis having reactive lymphadenopathy is quite common, close inspection reveal a punctate peripheral calcification associated with one of the nodes (green arrow in @Key Finding 1). Such calcifications should raise the suspicion for metastatic papillary thyroid cancer.The coronal image (@Key Finding 3) shows the elongated appearance of the right upper pole of the thyroid and the axial image shows a punctate calcification within this elongated region (@Key Finding 2). By imaging, this is extremely suspicious for underlying papillary thyroid cancer and metastatic lymphadenopathy, which were pathologically confirmed.But there's more to this case! Inspection of the lungs reveals pulmonary nodules (@Key Finding 4), both solid (for instance in the right upper lobe) and subsolid/groundglass (as seen in the left upper lobe). While the solid nodules would be suspicious for metastatic disease, the ground glass nodule is atypical. These were biopsied and proven to be pulmonary adenocarcinoma.
NeckCT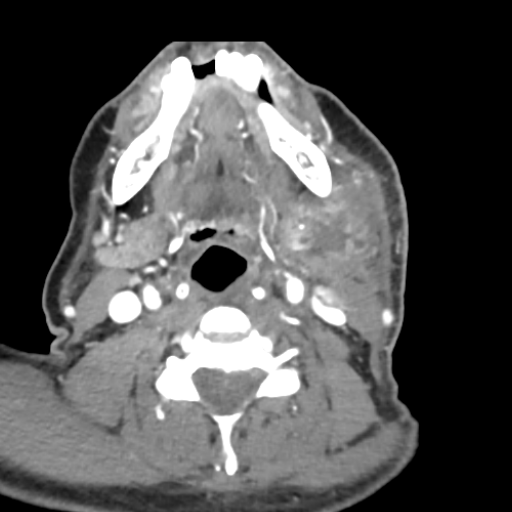
Submandibular space abscess (EDNeurorad Case 32)
107 views8 months agoThere is a multiloculated rim enhancing fluid collection within the left submandibular space (@Key Finding 1), which combined with the substantial surrounding stranding is consistent with an abscess. While most of the left submandibular gland has a normal appearance, superiorly (@Key Finding 2) the abscess and inflammation is indistinct from the gland and potentially arising focally from the gland. There is no sialolithiasis. There is additional thickening and asymmetric enhancement in the left oropharynx and palatine tonsil (@Key Finding 3), likely reactive as the epicenter of the major inflammation is clearly in the submandibular space.
NeckCT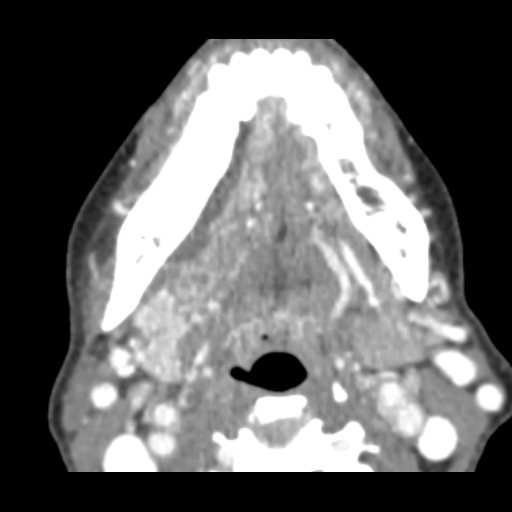
Odontogenic abscess (EDNeurorad Case 30)
128 views8 months agoThere is a right submandibular space fluid collection as shown on @Key Finding 1 and @Key Finding 2. There are numerous dental caries and periapical lucencies throughout but the first and third right mandibular molars are carious (red arrows @Key Finding 4), have periapical lucensies (green arrow @Key Finding 4), and are immediately adjacent to the fluid collection. @Key Finding 3 suggests contiguity of the fluid collection with the carious portion of the third mandibular molar. For odontogenic abscesses like this, do not rely on the presence of rim-enhancement to call an abscess. Abscesses can be small or thin and as such, not show rim enhancement. Any fluid collection next to a carious tooth with periapical lucency should be considered an odontogenic abscess until proven otherwise.
MaxillofacialCT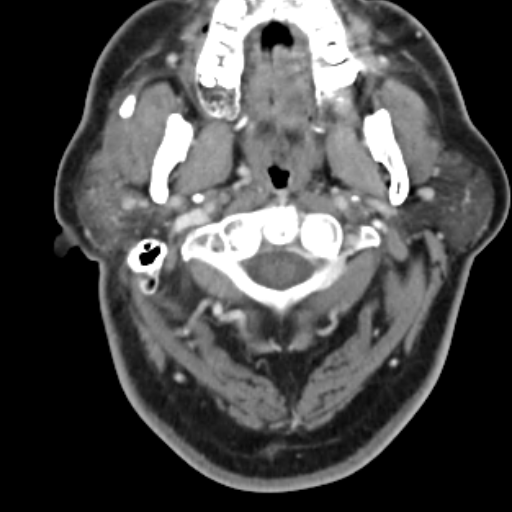
Parotiditis due to sialolithiasis (EDNeurorad Case 28)
107 views8 months agoThere is a stone within the proximal portion of the right parotid/Stensen's duct (red arrow @Key Finding 1). There is associated dilation of the proximal duct (white arrow @Key Finding 1) and if you window just right, you can see hyperenhancement of the duct mucosa. Finally, the right parotid gland is hyperdense compared to the left due to the edema and inflammation consistent with parotiditis (green arrow @Key Finding 1).
NeckCT
Instrumentation failure, infection (EDNeurorad Case 27)
134 views8 months agoThe patient is status post posterior decompression with instrumentation posterior fixation spanning from the occiput to the visualized thoracic spine. The occipital plate is inferiorly displaced compared to the bone and the three midline screws have all completely backed out and are in the soft tissues (red arrows in @Key Finding 1 and @Key Finding 2).Some additional findings include lucency throughout the length of the left C1 screw consistent with infection (@Key Finding 3) as well as a fluid collection in the posterior paraspinal tissues (@Key Finding 4). Such profound lucency and instrumentation failure should be considered highly suspicious for infection.
Cervical spineCT
Discitis Osteomyelitis (EDNeurorad Case 26)
172 views8 months ago@Key Finding 1 shows typical findings of discitis-osteomyelitis: loss of disc space with associated endplate erosions and destruction. In addition, as seen in @Key Finding 2, there is substantial surrounding paraspinal soft tissue swelling (red arrow) and osseus fragments (and likely epidural extension of the infection) within the spinal canal (green arrow). MRI without and with contrast would be the modality of choice to assess for any epidural abscess.
Lumbar spineCT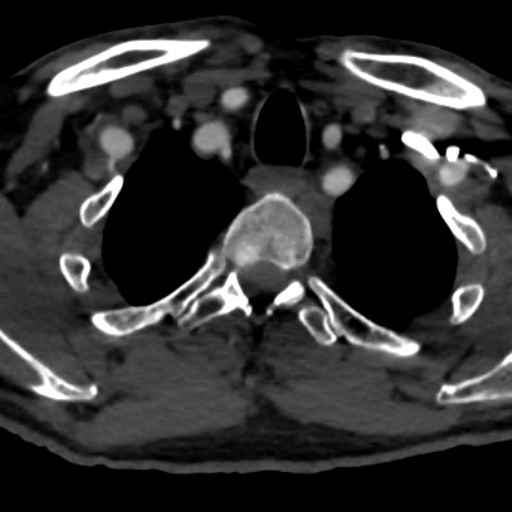
Traumatic right vertebral occlusion (EDNeurorad Case 25)
134 views8 months agoRight foramen transversarium fracture was noted on the prior case. The most proximal portion of the right vertebral artery near its origin is noted to be patent (@Key Finding 1). There is abrupt occlusion of the vessel shortly after this point (@Key Finding 2) and the vessel remains occluded thoughout the neck. Minimal opacification is present distally from collaterals.
Head and neckCTA