Loading...
Aggressive sinusitis with intracranial extension (EDNeurorad Case 15b)
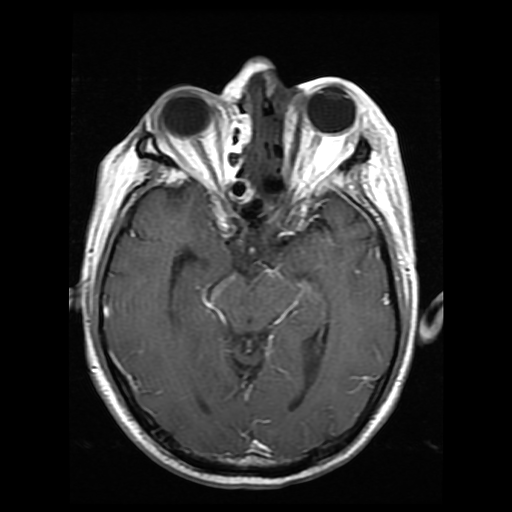
187 views8 months agoMR images confirm intracranial extension of sinusitis with DWI showing restricted diffusion in the gyrus recti (@Key Finding 1) and the T1 post showing thickening of the anterior dura on both sides (@Key Finding 2).The lack of enhancement in the thickening mucosa in the left ethmoid sinuses is suggestive of devitalized mucosa (@Key Finding 3). Additionally, there are remote areas of diffusion restriction, for instance shown in the bilateral superior frontal gyri (@Key Finding 4), that represent more widespread dissemination.T2 images also show the associated soft tissue infiltration as also shown on the CT images.
BrainMRI
Aggressive sinusitis with intracranial extension (EDNeurorad Case 15a)
169 views8 months agoThere is evidence of multifocal paranasal sinus inflammation with mucosal thickening. Involvement of the ethmoid sinuses is shown in @Key Finding 1. On @Key Finding 2, there is complete opacification of the left maxillary sinus but more importantly, there is stranding in the retromaxillary fat extending towards the lateral skin suggestive of aggressive sinusitis. Finally, and this is crucial to detect on imaging, @Key Finding 3 demonstrates hypoattenuation in bilateral inferior frontal lobes suggestive of intracranial extension of the infection with associated cerebritis.
HeadCT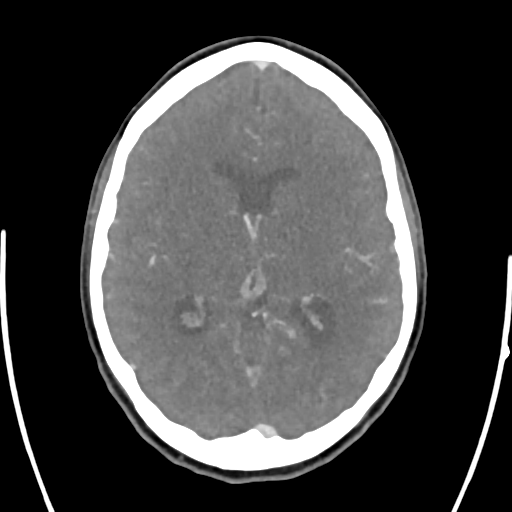
Thrombosis of straight sinus, inferior sagital sinus, vein of Galen, and internal cerebral veins (EDNeurorad Case 14b)
128 views8 months agoCTV corroborates the presence of thrombus within the vein of Galen (green arrow @Key Finding 1) extending to both internal cerebral veins (red arrows @Key Finding 2).Sagital reformation shows nicely how the thrombus extends from the straight sinus, towards the inferior sagital sinus and into the vein of Galen (@Key Finding 3).
HeadCTA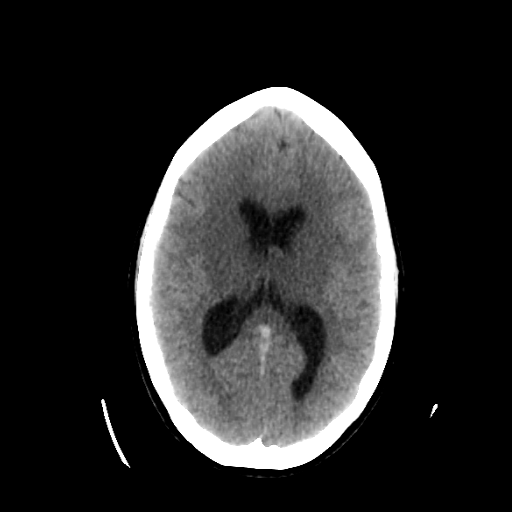
Thrombosis of straight sinus, inferior sagital sinus, vein of Galen, and internal cerebral veins (EDNeurorad Case 14a)
130 views8 months agoThere is hypoattenuation in the bilateral basal ganglia and thalami (red outline, @Key Finding 1). While this is a finding that can be seen in hypoxic-ischemic injury, the gray-white junction differentiation elsewhere is preserved. Closer inspection reveals hyperdense appearance at the junction of straight sinus, inferior sagital sinus and the vein of Galen (red arrow, @Key Finding 1) extending to the bilateral internal cerebral veins (green arrow, @Key Finding 2). This suggests that there is venous ischemia due to dural and internal venous thrombosis.
HeadCT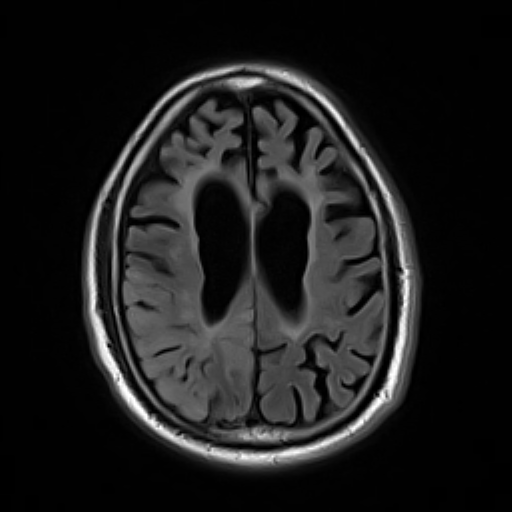
Seizure related signal abnormality (EDNeurorad Case 13b)
153 views8 months agoThe DWI and ADC images show gyriform diffusion restriction involving the right parietal and right occipital lobe (@Key Finding 1, @Key Finding 2). There is corresponding elevated FLAIR signal with cortical swelling (@Key Finding 3). Most notably, there is no elevation of TMAX (@Key Finding 4) despite the extensive region of cytotoxic edema which would be very odd for an infarct, in addition to the extensive combined MCA and PCA involvement. This patient had prolonged seizure activity accounting for these signal abnormalities. Neurological symptoms resolved after a few days corroborating the diagnosis.See: Characteristics of seizure-induced signal changes on MRI in patients with first seizures
BrainMRI
Infarct mimic (EDNeurorad Case 13a)
113 views8 months agoThere is loss of gray-white matter junction differentiation involving the right parietal (@Key Finding 1) and the right occipital lobe (@Key Finding 2). There is cortical swelling as evidenced by the profound effacement of the adjacent sulci compared to the left. Ordinarily, this would be consistent with a late acute infarct, however, this would require a combined right MCA and PCA territory vascular insult, which while possible, would be rare. See the followup case for further discussion.
HeadCT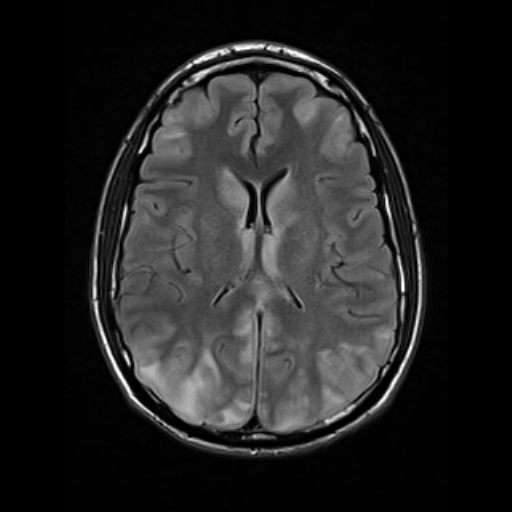
PRES (EDNeurorad Case 12b)
236 views8 months agoMR images more clearly depict the cortical and subcortical T2 hyperintensity with a posterior predominance (@Key Finding 1). The areas of signal abnormality demonstrated diffusion facilitation and not restriction as seen on ADC and are therefore, inconsistent with regions of acute infarction (@Key Finding 2). Note the better seen involvement of the bilateral caudate, medial thalami, and cerebella (@Key Finding 3). Patient symptoms as well as the signal abnormalities on imaging were reversible and resolved, corroborating the diagnosis of PRES.
BrainMRI
PRES (EDNeurorad Case 12a)
130 views8 months agoThere are patchy areas of subcortical and possibly cortical hypoattenuation (@Key Finding 1, @Key Finding 2). The regions of involvement include bilateral frontal lobes, posterior parietal lobes, parieto-occipital junctions, and posterior temporal lobes. Diagnostic considerations would include multifocal areas of ischemic injury but given the posterior predominace and subcortical location, also PRES.
HeadCT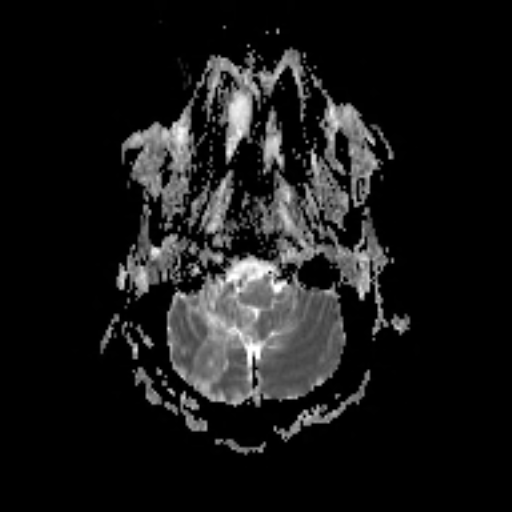
Retroclival meningioma with subacute right PICA territory infarct (EDNeurorad Case 11)
154 views8 months agoThe infarct is subacute in its timecourse: It has already pseudo-normalized on ADC (@Key Finding 1), has small areas of pre-contrast T1 hyperintensity (@Key Finding 2), and enhances (@Key Finding 3), all features characteristic of a subacute infarct.The retroclival extra-axial mass with homogenous enhancement is much better seen than on non-con CT (@Key Finding 4, @Key Finding 5)! A dural tail can be seen on the sagital image extending inferiorly and on the axial image extending to the left and towards the left internal auditory canal and the mass was proven to be a meningioma. On the T2 weighted images (@Key Finding 6), the mass is seen to compress the right vertebral artery against the medulla. It likely occluded or critically narrowed the right PICA resulting in the infarct.
BrainMRI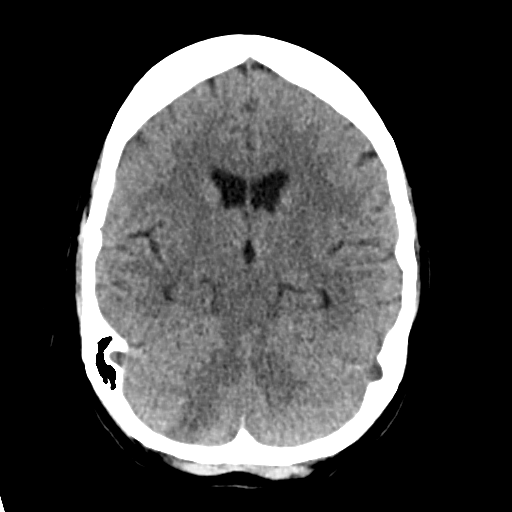
Right cerebellar infarct, clival meningioma (EDNeurorad Case 10)
139 views8 months agoThere is a wedge-shaped area of hypoattenuation with loss of gray-white differentiation in the right cerebellum consistent with an acute or early subacute infarct (@Key Finding 1). ---The much bigger finding, and surprisingly much more challenging to see due to the poor head positioning, is the large retroclival extra-axial mass that's compressing the medulla and pons (@Key Finding 2, @Key Finding 3)!
HeadCT