Loading...
Right M2 occlusion with right MCA infarct (EDNeurorad Case 9b)
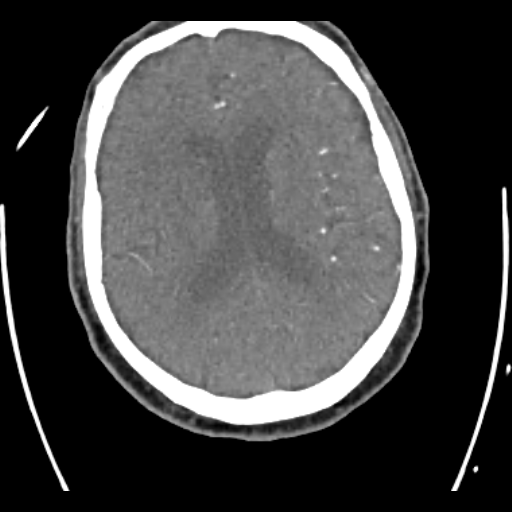
134 views8 months agoThere is a perfusion defect in the right parietal lobe with a wedge shaped area of elevated TMAX (@Key Finding 1), diminished CBF (@Key Finding 2), and relatively preserved CBV (@Key Finding 3). This pattern would typically be expected with an infarct that has salvagable tissue and not much infarct core.There is an associated right M2 branch occlusion with the occlusion at slice 367-368/510 on the CTA (@Key Finding 4). This matches nicely the location of the hyperdense M2 on the non-con head CT from Case 9a.As a bonus, did you catch the incidental mass in the deep lobe of the left parotid gland (@Key Finding 5)? It turned out to be a Warthin tumor.
Head and NeckCTA, CTP
Hyperdense right M2 (EDNeurorad Case 9a)
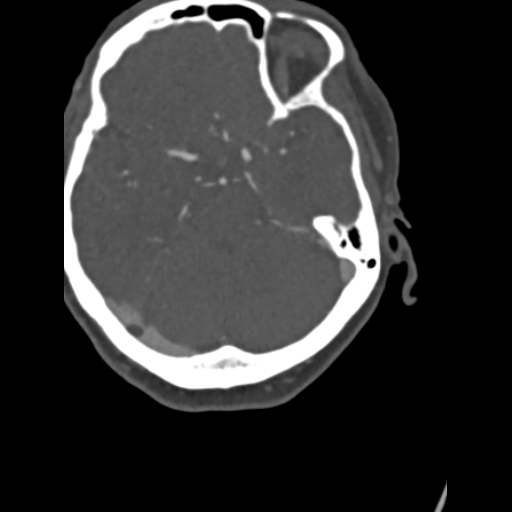
160 views8 months agoThere is a very prominent hyperdense right M2 branch within the sylvian fissure (red arrow, @Key Finding 1). The vascular nature of this can be confirmed by looking at the adjacent slices, particularly on the thin sections. This is suspicious for a thromus within an M2 branch of the MCA.
HeadCT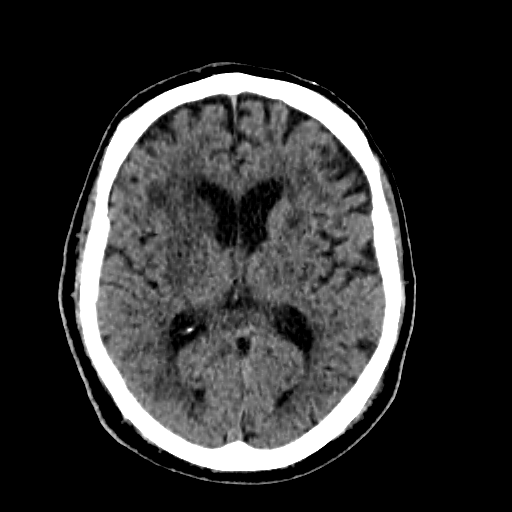
Right MCA stroke (EDNeurorad Case 8a)
164 views8 months agoWhen comparing the right basal ganglia to the left (@Key Finding 1, red outlined area compared to green outlined area), you will notice subtle hypoattenuation with loss of gray-white differentiation. This is typical of an acute infarct within the right MCA territory
HeadCT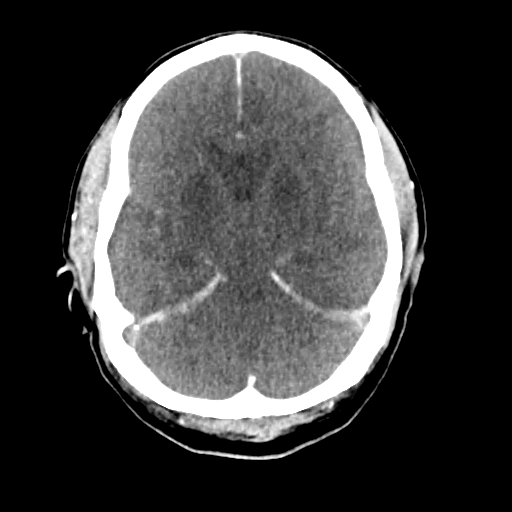
Hypoxic ischemic injury (EDNeurorad Case 7)
174 views8 months agoThere is hypoattenuation in the basal ganglia and thalami with loss of the normal gray-white differentiation (red outline, @Key Finding 1). There are findings of diffuse cerebral edema with effacement of all basilar cisterns, cerebral sulci, and the ventricles. In addition, there is a "pseudo-subarachnoid" hemorrhage appearance (green arrows) caused by the edematous and hypodense brain being in close apposition to the normal MCA and ACA branches which appear hyperdense. Notice also how hyperdense the dura (e.g. falx, tentoria) appear compared to the edematous brain. These are all findings of profound hypoxic ischemic injury.
HeadCT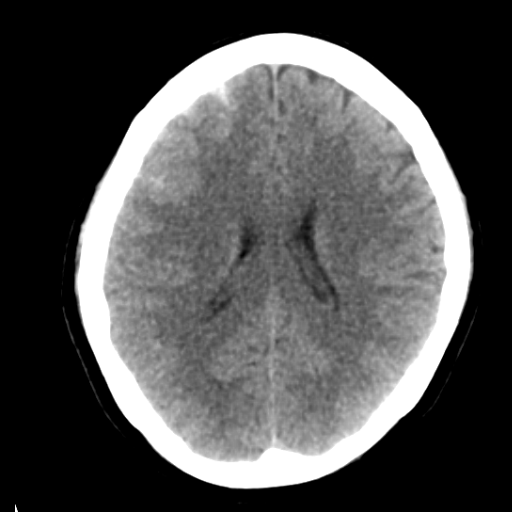
Intraparenchymal and subarachnoid hemorrhage (EDNeurorad Case 6)
164 views8 months agoThere is a small intraparenchymal hematoma with adjacent vasogenic edema in the right frontal lobe (red arrow, @Key Finding 1). Additional subarachnoid hemorrhage is seen in the adjacent frontal sulci (green arrows, @Key Finding 2). The etiology in this case is unclear.
HeadCT
Subtle subdural hematoma (EDNeurorad Case 5)
156 views8 months agoThere is a very small left convexity subdural hematoma, seen on multiple continuous slices (@Key Finding 1, @Key Finding 2). The best chance to catch this would be to use subdural windows (here I used width of roughly 150 and center of 80). The hematoma increased in conspicuity on subsequent head CTs.
HeadCT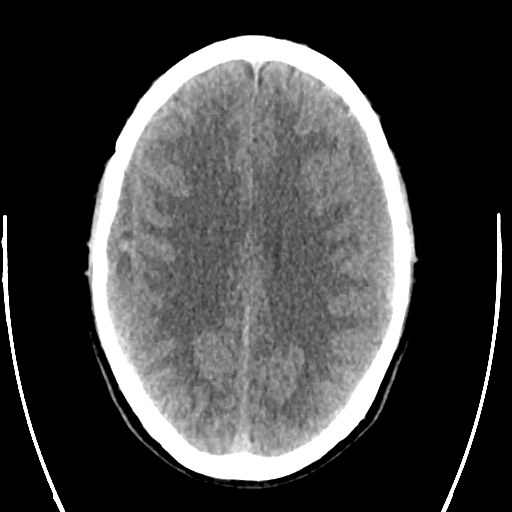
Subacute subdural hematomas (EDNeurorad Case 4)
154 views8 months agoThere are bilateral iso-attenuating subdural hematomas , consistent with a subacute time course (@Key Finding 1). The hematoma on the right has areas of hyperattenuation and is likely an acute on subacute hematoma. These are sizable hematomas, with some hyperattenuation on the right so they are relatively obvious to detect. For trickier cases, you need to pay careful attention to the cortex and notice areas of asymmetric apparent thickening and displacement, as seen here for the left sided hematoma.
HeadCT
Right subdural hematoma (EDNeurorad Case 3b)
172 views8 months agoClearly, there are post surgical changes from left subdural hematoma evacuation with a subdural drainage catheter in place (@Key Finding 1). However, there is now a lentiform extra-axial hematoma over the right parietal convexity, particularly evident on the coronal reformation (@Key Finding 2). The hematoma does not cross any sutures, although it is not large enough to approach the sutures yet. These imaging features are those of an epidural hematoma. The only odd aspect of this case is that there was no new trauma to cause an epidural hematoma. The hematoma was surgically confirmed to be in the subdural space so this is a great mimic case and an illustration that nothing is 100% accurate in imaging!Notice the additional subdural hematomas (@Key Finding 3) along the falx (green arrow), left tentorium (red arrow), and the right posterior fossa (red arrowhead).
HeadCT
Subdural hematoma (EDNeurorad Case 3a)
206 views8 months agoThere is a predominantly hyperdense left cerebral convexity subdural hematoma (@Key Finding 1). Near the vertex, there is a layering hematocrit level, typically seen in the setting of either active bleeding or coagulopathy (@Key Finding 2). The hematoma results in mass effect as evidenced by effacement of the left lateral ventricle compared to the right and midline shift.As nicely seen on the coronal reformations from the thin section data (@Key Finding 3), the hematoma has components along the left tentorium (red arrow) and the falx (green arrow). These can also be seen on the axial images.
HeadCT