Loading...
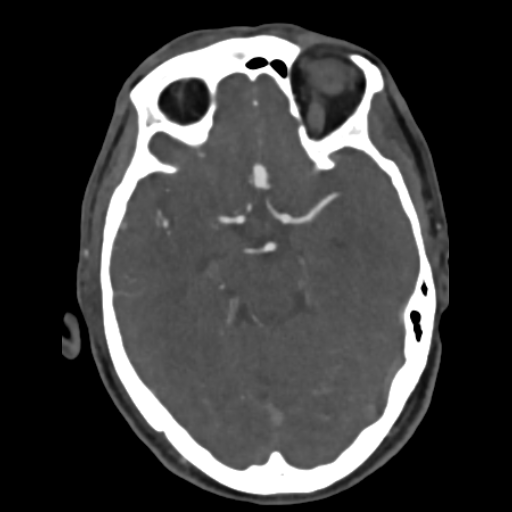
Ruptured ACoM aneurysm, additional left ICA terminus aneurysm (EDNeurorad Case V5, part 2)
52 views8 months agoCTA in this case shows an irregular anterior communicating aneurysm likely the source of the hemorrhage (@Key Finding 1). It also confirms the more "incidental" left ICA terminus aneurysm (@Key Finding 2).
Head and neckCTA
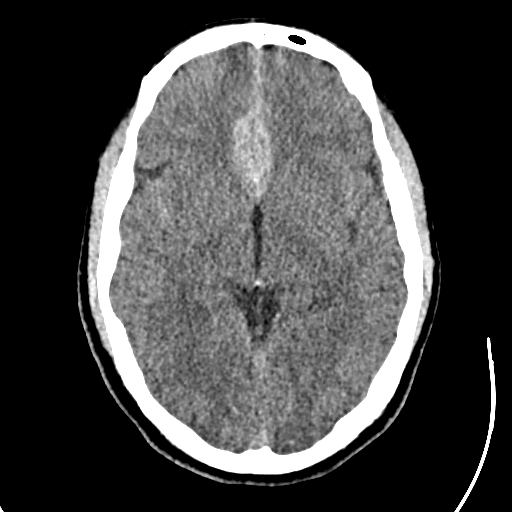
Likely aneurysmal SAH (EDNeurorad Case V5)
69 views8 months agoSubarachnoid blood in the interhemispheric region with a prominent clot in the pericallosal region suggestive of a distal A2 aneurysm (@Key Finding 1). Note that there is noncon evidence of a superiorly projecting aneurysm from the left terminal ICA (@Key Finding 2). You'll have to scroll up and down to convince yourself and also look at the coronal MPRs (@Key Finding 3).
HeadCT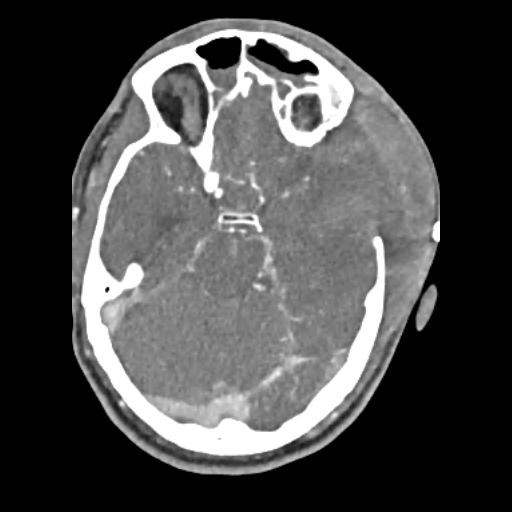
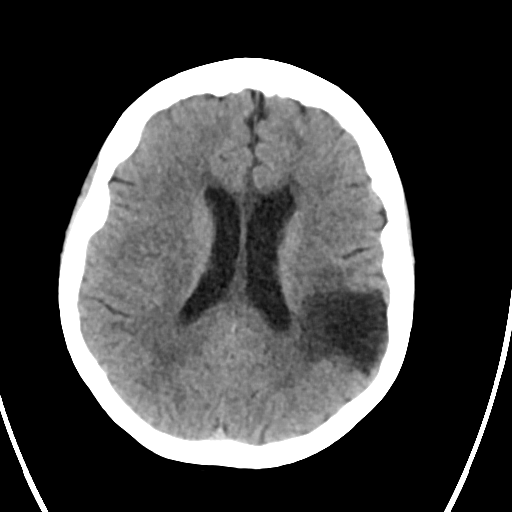
Extensive vasospasm (EDNeurorad Case V4, part 3)
68 views8 months agoInterval changes of left craniectomy with clipping of the ACoM aneurysm (red arrow @Key Finding 1). The craniectomy was likely performed because of the new parenchymal hematoma in the left temporal lobe with surrounding edema (blue arrow @Key Finding 1). There is some herniation of injured and edematous brain parenchyma through the craniectomy defect. Multifocal vasospams is seen. Axials show the severe spasm of the left ICA (@Key Finding 2) and basilar artery (@Key Finding 3) well. MIP images can be very valuable as well, showing the left ICA, MCA, and ACA spams (@Key Finding 4) as well as the bilateral right greater than left PCA spasm (@Key Finding 5).
HeadCTA
Ruptured ACoM aneurysm (EDNeurorad Case V4, part 2)
50 views8 months agoCTA confirms an elongated anterior communicating aneurysm as the source of the hemorrhage (@Key Finding 1). There is now extensive intraventricular extension of the hemorrhage with ventriculomegaly suspicious for developing hydrocephalus.
HeadCTA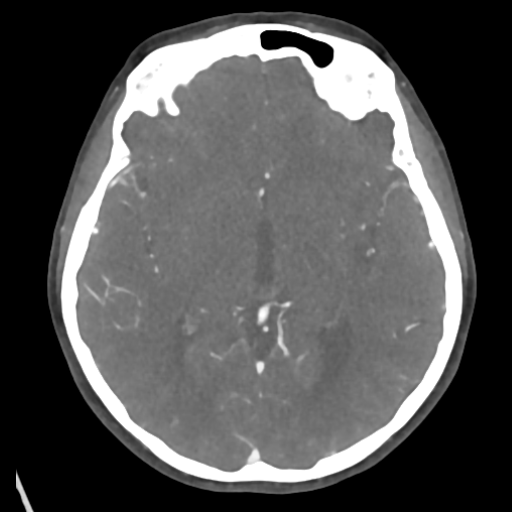
Left M3 occlusion (EDNeurorad Case V3, part 3)
59 views8 months agoMIP images show a filling defect in an M3 branch (@Key Finding 1) accounting for the slow flow seen on the prior FLAIR. This would be an extremely challenging call without having the MRI guiding us exactly where to look.
Head and neckCTA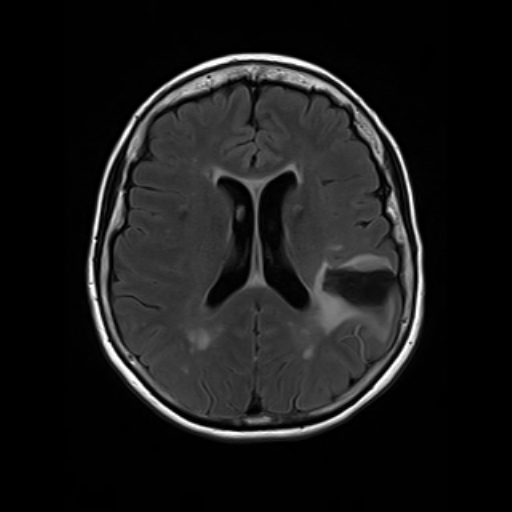
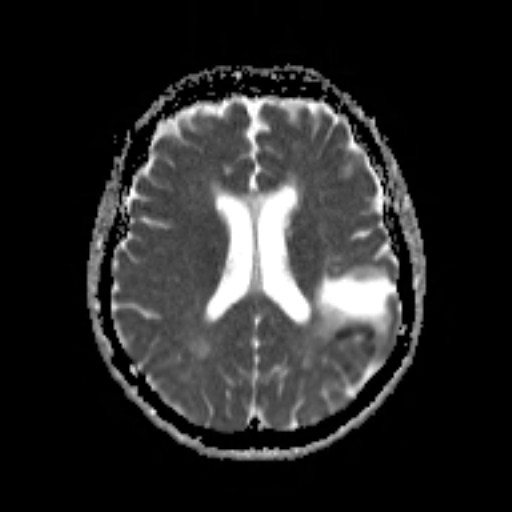
? acute left parietal infarct, MCA branch slow flow (EDNeurorad Case V3, part 2)
70 views8 months agoBorderline high DWI signal (@Key Finding 1 pretty equivocal at this point). However, FLAIR hyperintense vessels in the adjacent MCA branches (@Key Finding 2) suggesting slow flow due to a proximal stenotic lesion. An MRA or CTA should be obtained.
BrainMRI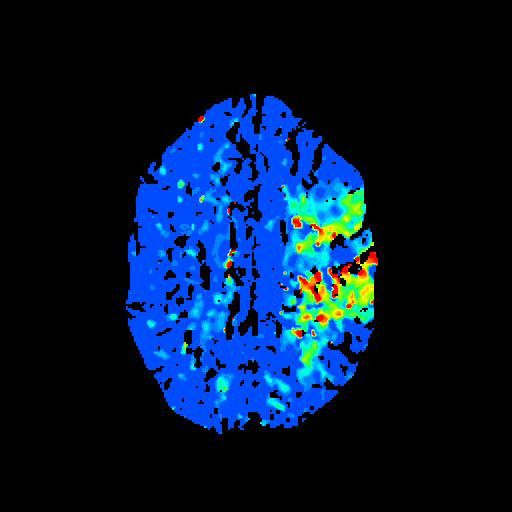
Left M2 occlusion with matched infarct (EDNeurorad Case V1, part 2)
54 views8 months agoMatched defect shown on perfusion images (CBF for core @Key Finding 1, and TMAX for at risk tissue @Key Finding 2).Associated distal M2 occlusion (@Key Finding 3 arrow right before occlusion, scroll up and down to confirm).
Head and neckCTA, CTP