Loading...
ACA (likely azygous) occlusion (EDNeurorad Case V13, part 3)
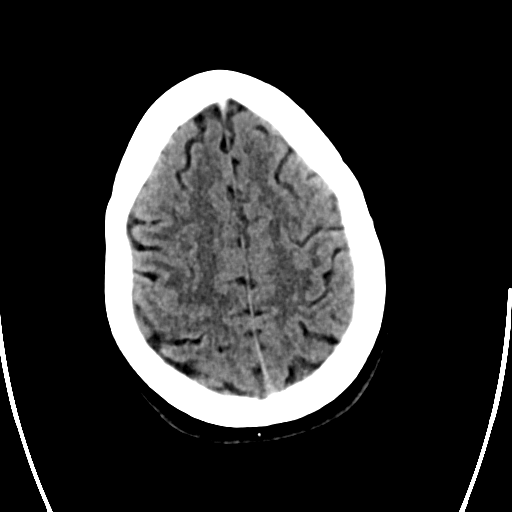
71 views8 months agoThere's occlusion of the ACA, which is possibly singular (i.e. azygous) given that it looks pretty large (@Key Finding 1). You can actually see the thrombus filled occluded distal segment with calcifications along its periphery.
Head and neckCTA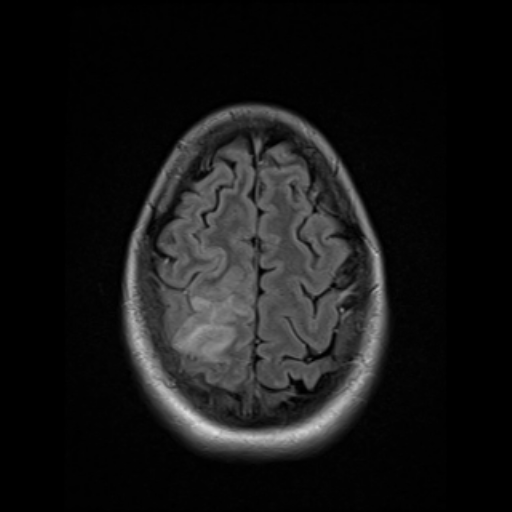
Venous infarct due to superior sagittal sinus thrombosis (EDNeurorad Case V11, part 3)
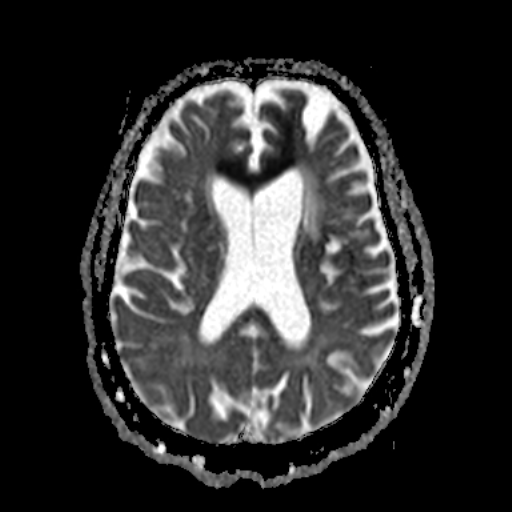
76 views8 months agoThis is just to show correlative MR findings of a venous infarct. Note that while there is high DWI signal (@Key Finding 1), it's not really restricting when seen on ADC and is just T2 shinethrough (@Key Finding 2). This is pretty typical of venous infarcts. The region developed encephalomalacia on followup so it is an infarct and not just edema from venous congestion. SWI images show susceptibility from the thrombus in the superior sagittal sinus and adjacent cortical veins (@Key Finding 3). MRV just shows correlative but unchanged findings as the CTA.
BrainMRI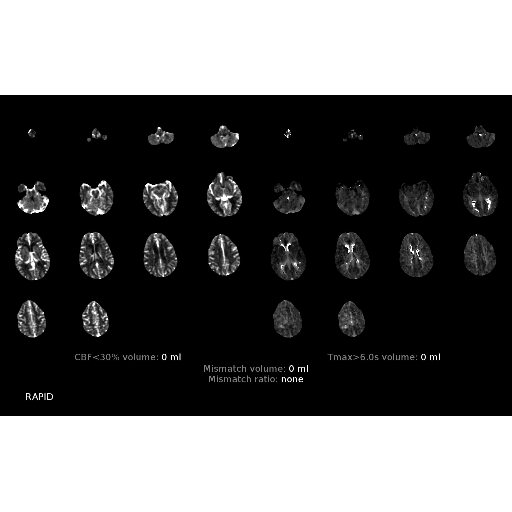
Dural venous sinus thrombosis with venous infarct (EDNeurorad Case V11, part 2)
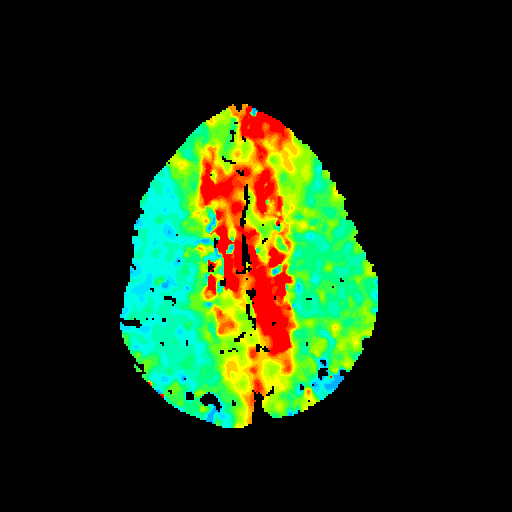
46 views8 months agoPerfusion images are very suboptimal here as they don't go high enough to cover the bulk of the infarct! You see a subtle area of marginal TMAX deficit at the inferior aspect of the infarct (@Key Finding 1).CTA shows no arterial problem but there is thrombosis of the superior sagittal sinus with thrombus also in the adjacent cortical veins (@Key Finding 2).
Head and neckCTA, CTP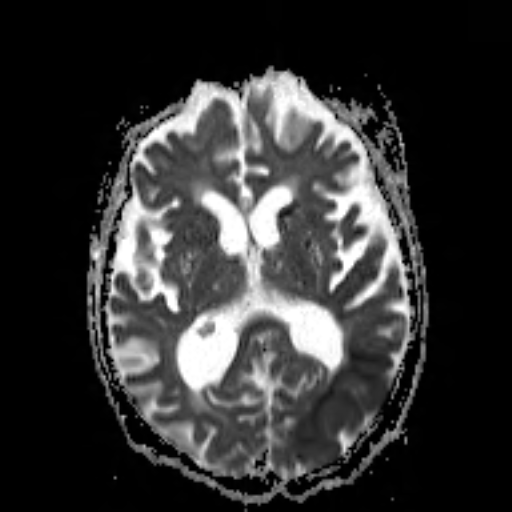
Acute infarcts due to acute calcified emboli from left ICA (EDNeurorad Case V10, part 3)
59 views8 months agoDWI images show multifocal areas of left hemispheric acute infarctions (@Key Finding 1). SWI images show susceptibility artifact corresponding to several of the emboli (@Key Finding 2).
BrainMRI
Age indeterminate emboli likely from left ICA, matched infarct (EDNeurorad Case V10, part 2)
50 views8 months agoPerfusion images show a relatively matched infarct in the left occipital lobe. --- CTA confirms intra-arterial location of some of these calcification (for instance panel A red arrow) with associated diminished upstream and downstream opacification. It also confirms fetal type left PCA (panel A blue arrow). There is a heavily calcified and somewhat irregular shaped plaque in the left carotid bifurcation (panel B orange arrow) that may be the source of both the PCA and MCA emboli.
Head and neckCTA, CTP
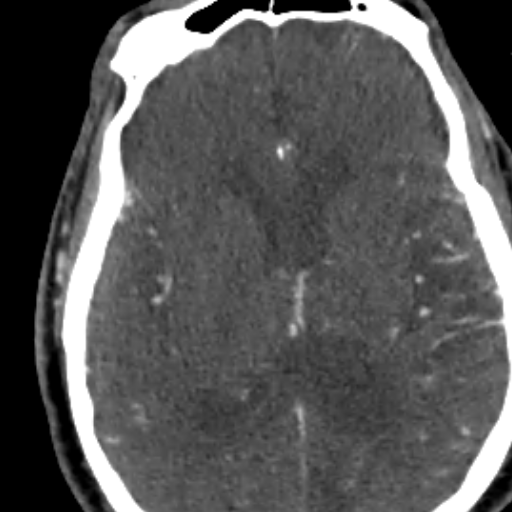
Age indeterminate calcified emboli (EDNeurorad Case V10)
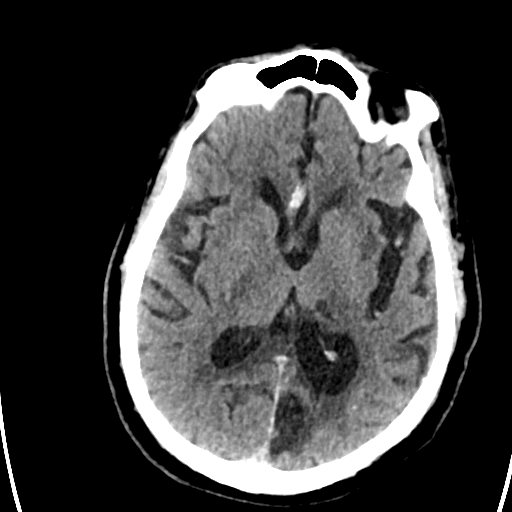
48 views8 months agoThere is no hemorrhage or clear loss of grey-white. However, there are numerous calcification within the sulci of the left cerebral hemisphere. These are almost certainly in the arterial branches in both the PCA (@Key Finding 1) and MCA (@Key Finding 2) distribution (there are many more beyond the two highlighted here). These would be consistent with age-indeterminate calcified emboli. Atherosclerotic disease is unlikely given the strikingly unilateral nature of the findings. The combined PCA + MCA distribution should make one think of a left carotid source with fetal type PCA circulation.
HeadCT