Loading...
Acute on chronic critical cervical ICA stenosis (EDNeurorad Case V17, part 2)
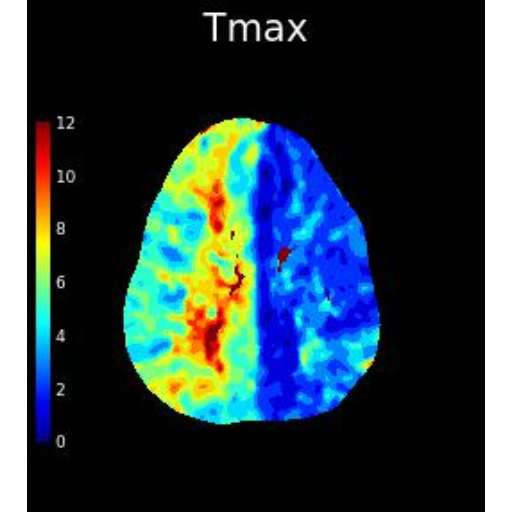
62 views8 months agoCTA shows no intracranial occlusion or stenosis. There is calcified and noncalcified plaque at the right cervical ICA resulting in severe stenosis (@Key Finding 1).@Key Finding 2 shows a large TMAX deficit in the right MCA/ACA and MCA/PCA borderzone without a calculated infarct core (you can see a matched defect on the left corresponding to old infarct). Given the above high grade right carotid stenosis, we can compare MTT to TMAX to see if we're dealing with a compensated delayed transit or an acute on chronic insult. While the MTT is much more normal than TMAX, there are a few regions where there is also an MTT deficit (@Key Finding 4) consistent with acute on chronic hemodynamic compromise.
Head and neckCTA, CTP
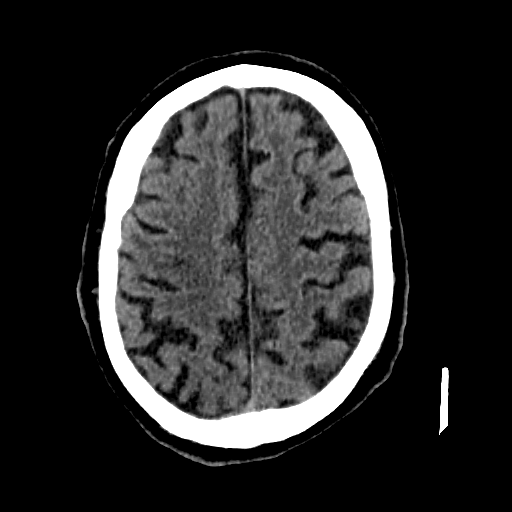
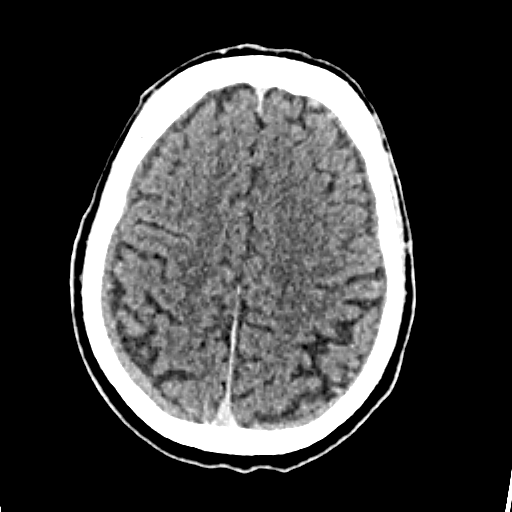
No hemorrhage (EDNeurorad Case V17)
68 views8 months agoOld left MCA infarcts. A few nonspecific subcortical hypodensities in the right MCA territory (@Key Finding 1), can certainly be chronic microvascular ischemic change but there's a reason they're called nonspecific as we'll see in this case!
HeadCT
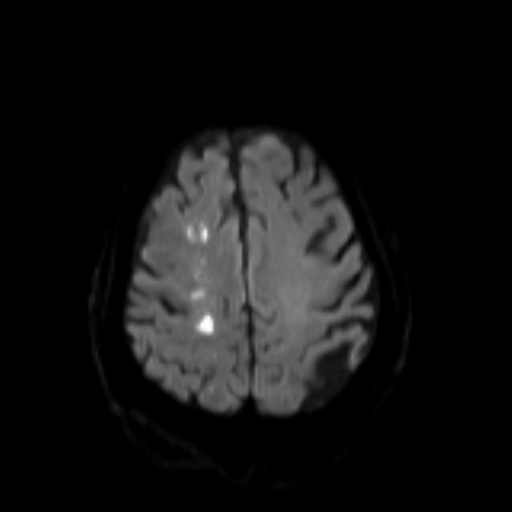
Acute on chronic basilar occlusion (EDNeurorad Case V16, part 4)
59 views8 months agoDWI shows acute infarcts in bilateral cerebellum (@Key Finding 1), brainstem (@Key Finding 2), and left thalamus (@Key Finding 3). MRA actually does a good job of showing that the right vert is not fully occluded but rather stenotic (@Key Finding 4).
BrainMRI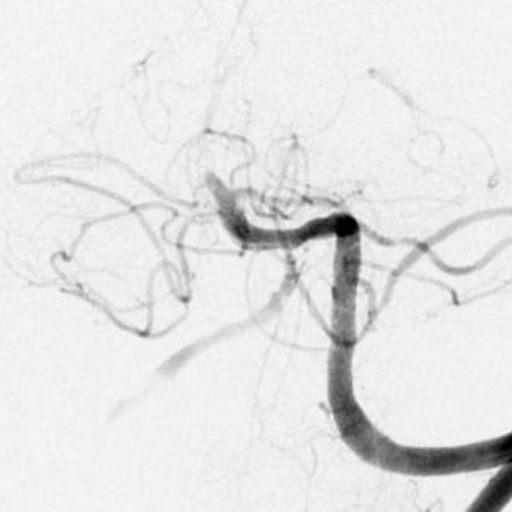
Basilar occlusion on severe atherosclerotic disease (EDNeurorad Case V16, part 3)
65 views8 months agoLeft vert injection (@Key Finding 1) shows occluded basilar artery and moderate stenosis of the right vert at insertion to the basilar. Left vert injection after thrombectomy and stenting of the basilar shows residual moderate to severe basilar stenosis (@Key Finding 2) as well as multifocal additional atherosclerotic disease. This was an acute on chronic problem.
HeadAngiogram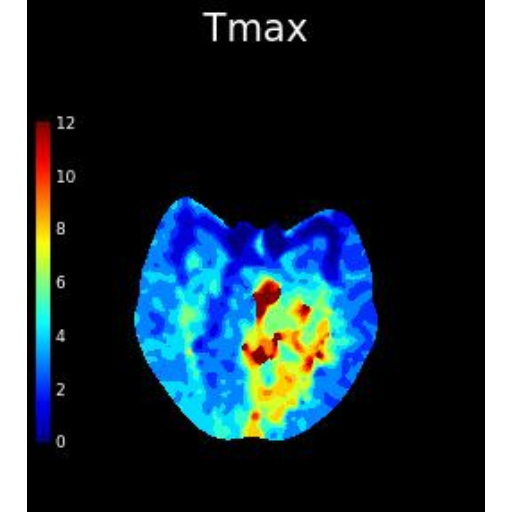
Basilar occlusion, acute on chronic (EDNeurorad Case V16, part 2)
53 views8 months agoThe summary RAPID calculations show a large region of ischemic at risk parenchyma consisting of the entire brainstem and cerebellum as well as the left occipital lobe (@Key Finding 1). No infarct core is detected by RAPID. There is basilar occlusion as seen on CTA discussed below. If there is any question about whether the TMAX deficit represents simple delayed contrast transit as a result of some upstream stenosis/occlusion that is otherwise chronic and compensated, looking at MTT can help. If MTT is also abnormal (as is the case here @Key Finding 3) the perfusion deficit is more likely to represent an acute on chronic hemodynamic decompensation.There is occlusion of the basilar artery (red arrow @Key Finding 4). There is no opacification of the distal right vertebral artery (blue arrow @Key Finding 5 - as it turns out this one is not occluded but just severely narrowed at insertion to the basilar and so the apparent lack of opacification is purely flow related). The left PCA is not clearly opacified compared to the robust right PCA (@Key Finding 6) due to fetal type origin of the right PCA.
Head and neckCTA, CTP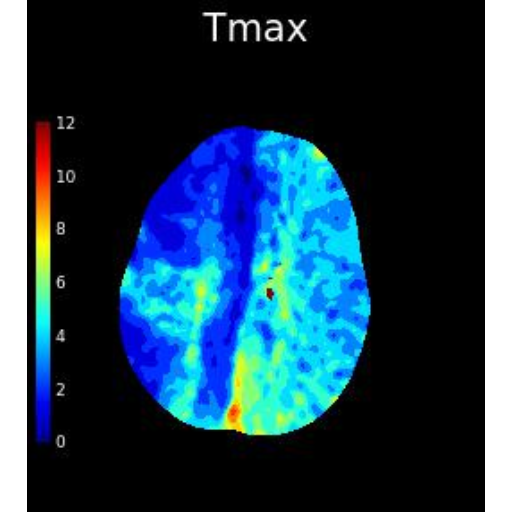
Seizure related perfusion changes (EDNeurorad Case V15, part 2)
48 views8 months agoRAPID has detected some TMAX deficits which when you look at the slightly lower threshold of 4s (blue region in the summary panel @Key Finding 1) looks very nonvascular and likely artefactual. Looking at the TMAX images, however, you will see that the striking abnormality is how low TMAX is in the right hemisphere (with some sparing of the primary motor and somatosensory cortices @Key Finding 2). Identifying that the abnormal side is the right side, you can tell that the assymetries in the CBF and CBV imply that there is increased perfusion to the right hemisphere (and not decreased perfusion to the left).CTA images show no vascular occlusion but early venous opacification throughout the right hemisphere (@Key Finding 3), matching the conclusion from perfusion that there is elevated perfusion and blood flow to the right. This person was in status epilepticus (subclinical) at the time of the CTA/CTP with seizure onset in the right hemisphere based on EEG obtained 30 minutes later. Remember seizures (and migraines) when you have odd perfusion patterns such as this case.
Head and neckCTA, CTP