Loading...
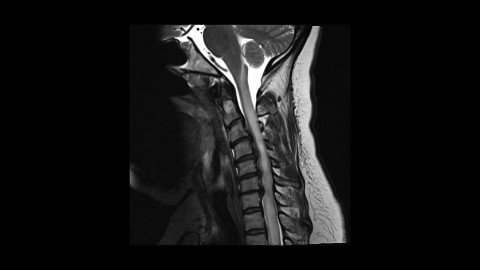
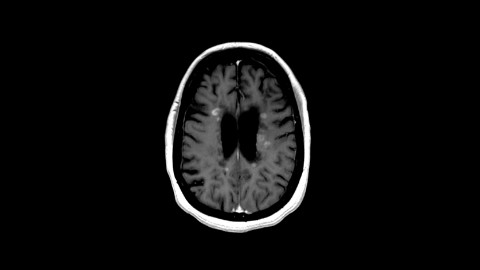
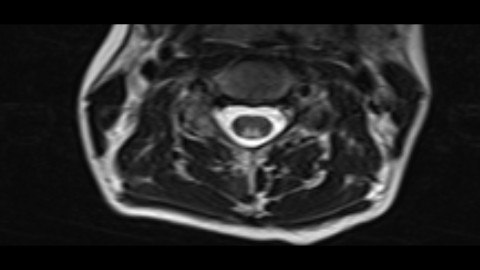
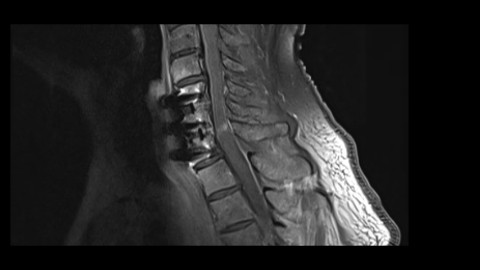
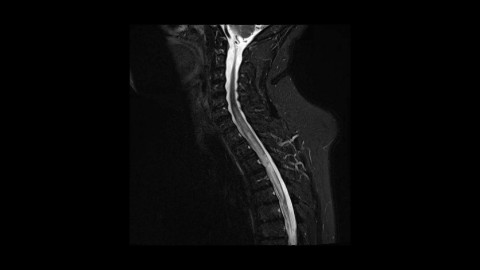
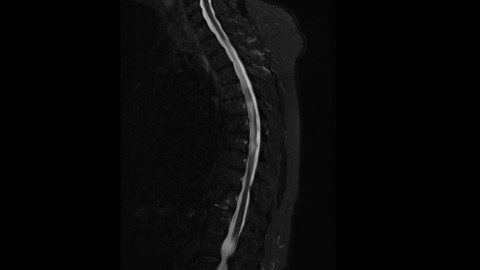
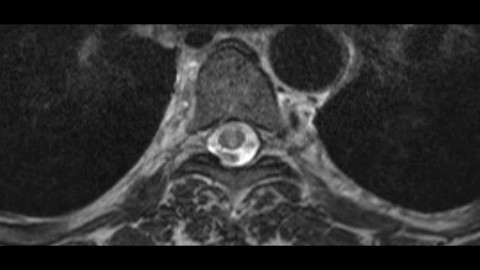
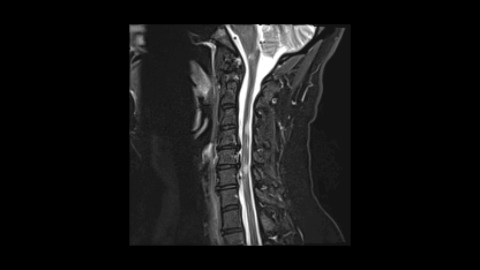
Spondylotic Myelopathy with enhancement
156 views7 months agoThis is a case of spondylotic myelopathy presenting with longitudinally extensive myelopathy extending both above and below the levels of spinal cord compression as well as pronounced enhancement. Post decompression images show marked improvement of the T2 hyperintensity and resolution of the enhancement. Keep this pattern of spondylotic myelopathy in mind as it can be mistaken for demyelinating diseases or even tumors.
SpineMRI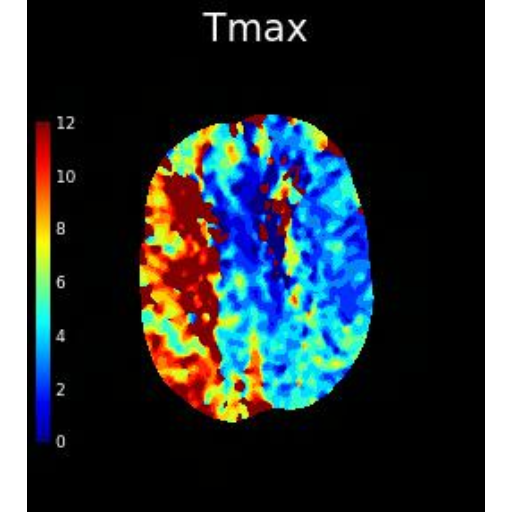
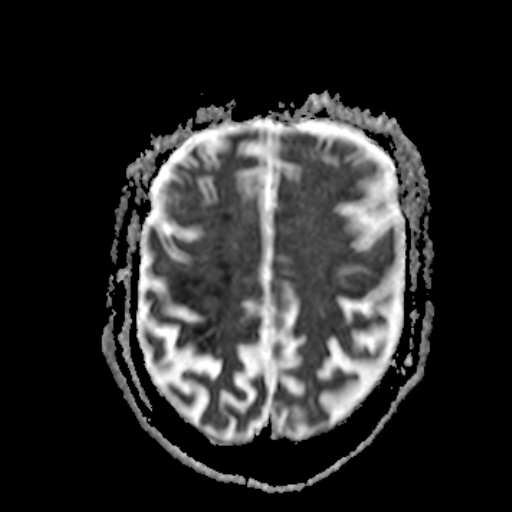
Acute on chronic critical right ICA stenosis (EDNeurorad Case V18, part 2)
66 views8 months agoExtensive intra- and extra-cranial atherosclerotic disease but no large vessel intra-cranial occlusion. There is critical narrowing of the right proximal ICA due to a mixed calcified and non-calcified plaque (@Key Finding 1).RAPID summary (@Key Finding 2) shows a large mismatched defect in the right MCA and posterior circulation without a core making it difficult to know whether this is a chronic compensated state or if there is a superimposed acute insult. MTT is more symmetric but the right side appears to have asymmetrically greater MTT prolongation (@Key Finding 3) so this can be taken as perfusion evidence suggestive of a superimposed acute insult. Of course the most definite evidence was from the head CT which pretty clearly showed a likely area of peri-rolandic acute infarction.
Head and neckCTA, CTP