Loading...

Hyperacute stroke from CPAISD (002)
108 views7 months agoCase taken from the CPAISD dataset. The dataset consists of non contrast Head CTs obtained as part of a hyperacute stroke workup. The workup for all patients included CTA and CT perfusion, although CTA and CTP series are not made publicly available. The CT perfusion is used to generate "ground truth" segmentations of ischemic penumbra and infarct core. You can enable these segmentations by clicking @Labels (once you enable them, you can toggle their visibility with the keyboard shortcut "a"). Many of the non contrast head CTs have nice CT correlates of hyperacute stroke and you can use the segmentations to guide you to them. Leave a comment with any findings you see and the slice number!Citation (attribution required if you use the case):Umerenkov, D., Kudin, S., Peksheva, M. et al. Core-Penumbra Hyperacute Ischemic Stroke Dataset. Sci Data 12, 707 (2025). https://doi.org/10.1038/s41597-025-05000-0 (https://doi.org/10.1038/s41597-025-05000-0)
HeadCT
Hyperacute stroke from CPAISD (001)
142 views7 months agoCase taken from the CPAISD dataset. The dataset consists of non contrast Head CTs obtained as part of a hyperacute stroke workup. The workup for all patients included CTA and CT perfusion, although CTA and CTP series are not made publicly available. The CT perfusion is used to generate "ground truth" segmentations of ischemic penumbra and infarct core. You can enable these segmentations by clicking @Labels (once you enable them, you can toggle their visibility with the keyboard shortcut "a"). Many of the non contrast head CTs have nice CT correlates of hyperacute stroke and you can use the segmentations to guide you to them. Leave a comment with any findings you see and the slice number!Citation (attribution required if you use the case):Umerenkov, D., Kudin, S., Peksheva, M. et al. Core-Penumbra Hyperacute Ischemic Stroke Dataset. Sci Data 12, 707 (2025). https://doi.org/10.1038/s41597-025-05000-0 (https://doi.org/10.1038/s41597-025-05000-0)
HeadCT
Carotid cavernous fistula
927 views7 months agoThere is right sided proptosis and some periorbital preseptal stranding. Possible minimal post-septal stranding. Certainly orbital cellulitis is a diagnosis to be entertained, if the presentation was suggestive of an infection. However, there is a crucial additional finding here that the proptosis is out of proportion to any inflammation and the right superior ophthalmic vein is substantially larger than the left (@Key Finding 1). This appearance can be seen with carotid cavernous fistulization (CCF) or thrombosis and should be assessed.The best next step when there is suspicion for CCF is a non-con TOF MRA as it nicely suppresses venous signal. CTA is an option but very often, there is venous contamination which will make assessment for abnormal arterial to venous connection difficult.In this case, a CTA was obtained. High flow carotid cavernous fistula is confirmed (@Key Finding 2) since there is clear and robust arterial phase opacification of the right cavernous sinus (red arrow) AND no venous contamination (no contrast in the superior sagittal sinus for instance, blue arrow).Incidentally, there are also bilateral chronic subdural hematomas (@Key Finding 3).
HeadCT, CTA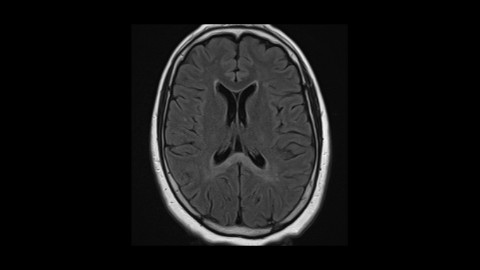
Neuromyelitis optica (optic neuritis + cord lesion + intracranial lesion)
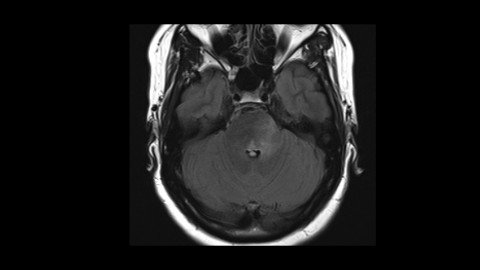
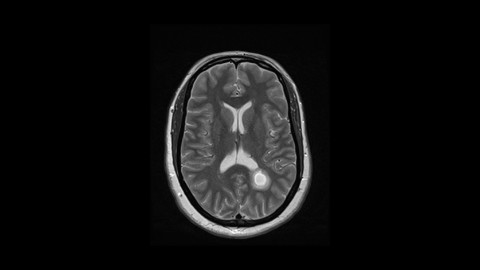
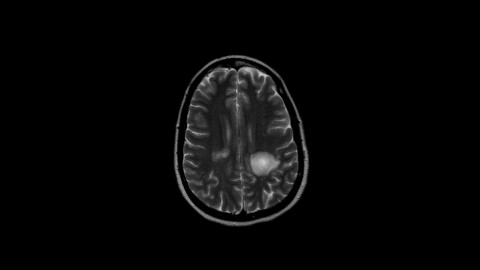
128 views7 months agoNice case showing typical features of NMO including optic neuritis (@Key Finding 2), longitudinally extensive cord myelitis (@Key Finding 3, @Key Finding 4), and peri-ependymal corpus callosal lesion (@Key Finding 1, note the confluent nature as opposed to the focal abnormalities in MS)
Brain Spine OrbitsMRI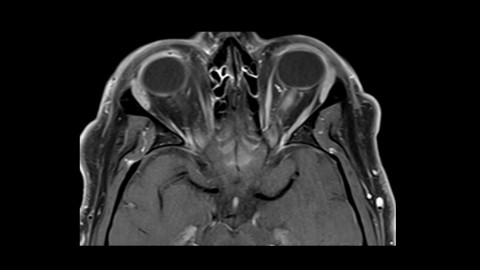
Multiple Sclerosis with Optic Neuritis
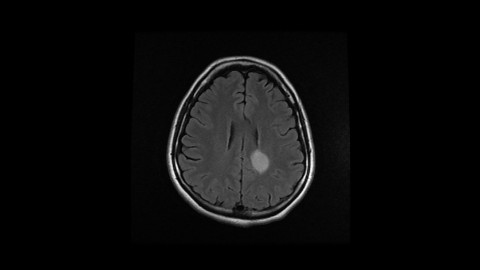
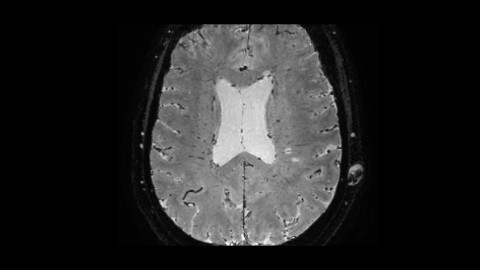
132 views7 months agoA case of multiple sclerosis with active left sided optic neuritis (@Key Finding 1, @Key Finding 5). Notice that the patient has MS lesion in the periventricular (@Key Finding 4) and infratentorial (@Key Finding 3) distribution so meets dissemination in space.
Brain OrbitsMRI