Loading...
Colon Cancer PET/CT (case 983827-000035 from PETWB-REP)
0 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Colon Cancer taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression a. Thickening of the intestinal wall at the junction of the descending colon and sigmoid colon with increased FDG metabolism suggests colon cancer; please refer to pathology reports. b. Metastasis to the mesenteric and adjacent left pelvic lymph nodes around the lesion is possible. Reactive hyperplasia of the retroperitoneal and bilateral inguinal lymph nodes is highly probable. a. Several ground-glass nodules in the apical segment of the right upper lobe, the apical-posterior segment of the left upper lobe, and the posterior-basal segment of the left lower lobe, with normal FDG metabolism, suggest chronic inflammatory nodules or atypical adenomatous hyperplasia; please refer to annual follow-up HRCT. b. Scattered chronic inflammation and remnants in both lungs. Slightly low-density nodule under the capsule of the right lobe of the liver, with background FDG uptake, suggests a possible hemangioma; ultrasound or MRI follow-up is recommended; multiple liver cysts. Septated gallbladder possible, cholecystitis with stones. Chronic gastritis, chronic duodenal bulb inflammation. Partial vertebral osteophyte formation. L4/5 and L5/S1 intervertebral disc bulging. A mass in the sellar region with elevated FDG metabolism strongly suggests a pituitary tumor; a follow-up enhanced MRI of the pituitary gland is recommended. Postoperative changes after nasal polyp surgery; chronic inflammation of the bilateral ethmoid sinuses, maxillary sinuses, and part of the nasal mucosa; and likely chronic inflammation of the nasopharynx and bilateral palatine tonsils. Specialist follow-up is recommended for all of the above. Bilateral reactive hyperplasia of cervical lymph nodes. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT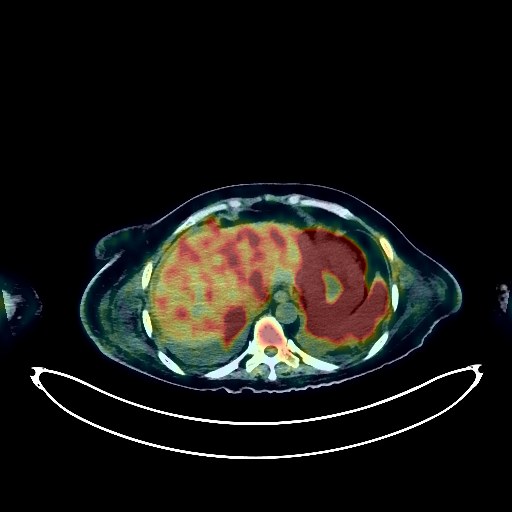
Lymphoma PET/CT (case 983827-000202 from PETWB-REP)
0 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Lymphoma taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression a. Multiple lymphadenopathy throughout the body with increased FDG metabolism (see description for details); multiple nodular soft tissue density shadows in the abdominopelvic cavity with increased FDG metabolism; b. Extensive and irregular thickening of the gastric wall with increased FDG metabolism; thickening of the small intestine wall in the midline of the pelvis with increased FDG metabolism; c. Multiple low-density lesions under the liver capsule with increased FDG metabolism; splenomegaly with increased FDG metabolism; space-occupying lesion in the right adrenal region with increased FDG metabolism; d. Multiple nodular and patchy soft tissue density shadows in the subcutaneous soft tissue and muscles throughout the body with increased FDG metabolism; heterogeneous increased FDG metabolism in the bone marrow cavity throughout the body. Based on the medical history, all of the above suggest multisystemic lymphoma infiltration. Follow-up after treatment is recommended. Uneven density in the left and right lobes of the thyroid gland; low-density nodule with calcification in the left lobe; increased FDG metabolism; thyroid cancer to be ruled out; further ultrasound examination recommended. Chronic inflammatory lesions in the upper lobes of both lungs. Scattered fibrotic lesions in both lungs. Bilateral pleural effusion; partial atelectasis in the lower lobes of both lungs. Anemia changes; partial calcification of arterial walls (including coronary arteries). PICC line inserted. Calcification in the right breast. Possible intrahepatic hemangioma; comprehensive analysis with contrast-enhanced MRI recommended. Cholelithiasis. Complex cyst in the left kidney. Urinary catheter inserted. Post-hysterectomy changes. Small amount of pelvic effusion. Degenerative changes in the spine; L4/5 and L5/S1 intervertebral disc bulge. Subcutaneous edema in the abdomen and buttocks. Cranial scintigraphy showed no obvious abnormalities. Chronic sphenoid sinusitis. Osteoma of the right frontal bone. Benign bone lesion of the right parietal bone. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT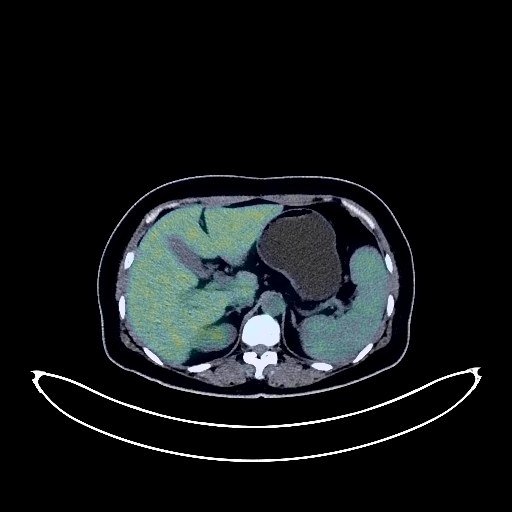
Cervical Cancer PET/CT (case 983827-000071 from PETWB-REP)
0 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Cervical Cancer taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression a. Cervical mass with increased FDG metabolism, consistent with cervical cancer. Multiple lymph node metastases bilaterally to the iliac vessels and in the retroperitoneum. Metastasis to the left supraclavicular fossa lymph nodes is highly likely; follow-up is recommended. b. Uterine fibroids are highly likely, possibly due to physiological uptake within the uterine cavity; bilateral ovarian cysts. Ultrasound follow-up is recommended. Chronic inflammatory nodules in the upper and middle lobes of the right lung; CT follow-up is recommended to rule out other confounding nodules. A few post-inflammatory lesions in both lungs. Anemia changes, slight arteriosclerosis in some arteries. Angiomyolipoma of the left kidney. Calcification in the right lobe of the liver. Splenomegaly, accessory spleen. Residual contrast agent in the urinary tract. Chronic inflammatory changes in the cardia and antrum of the stomach. a. Mild osteophyte formation in the spine, L4/5 and L5/S1 intervertebral disc herniation, calcification at the posterior margin of the L5/S1 intervertebral disc. b. Osteitis condensans of the bilateral sacroiliac joints. Increased FDG metabolism throughout the bone marrow cavity, suggestive of reactive proliferative changes. No obvious abnormalities were found on cranial scintigraphy. Chronic inflammation of both maxillary sinuses. Inflammation of the left upper and lower alveolar ridges. Reactive hyperplasia of both cervical lymph nodes. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT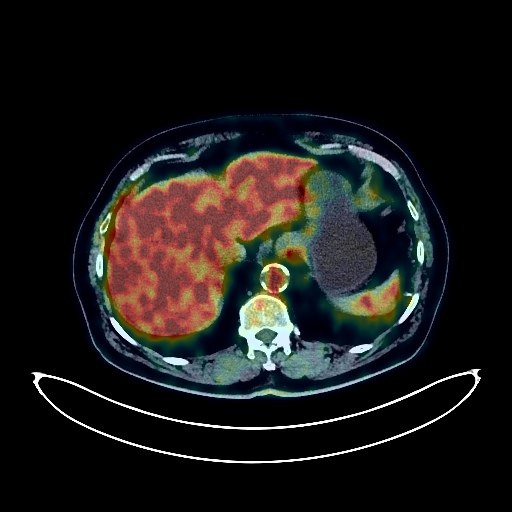
Lung Cancer PET/CT (case 983827-000083 from PETWB-REP)
0 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Lung Cancer taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression a. A mass in the posterior segment of the left upper lobe with elevated FDG metabolism, suggestive of lung cancer, most likely small cell lung cancer; multiple lymph node metastases in the left hilum and mediastinum. b. Some solid nodules in the left upper lobe with mildly elevated FDG metabolism, suggestive of metastatic tumors; chronic inflammatory nodules in the right upper lobe and left lower lobe are more likely. Follow-up with CT is recommended. c. Metastatic tumor in the upper right humerus. Emphysema with bullae in both upper lobes. Scattered post-inflammatory lesions in both lungs. Slight thickening of the left pleura. Calcification of some arterial walls (including coronary arteries). Post-bilateral carotid artery stenting. Post-cholecystectomy with common bile duct stones. Left adrenal hyperplasia. Cysts in the left and right renal pelvis. Calcifications in the prostate. Small amount of hydrocele in both testes, with calcification on the left. Chronic inflammatory changes in the gastric antrum. Degenerative changes in the spine, with L3/4, L4/5, and L5/S1 intervertebral disc bulging accompanied by pneumoconiosis and degeneration. Age-related brain abnormalities, with chronic sublaminal effusion and hemorrhage on the right frontoparietal side, and deep lacunar ischemic lesions in the brain; follow-up MRI is recommended. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT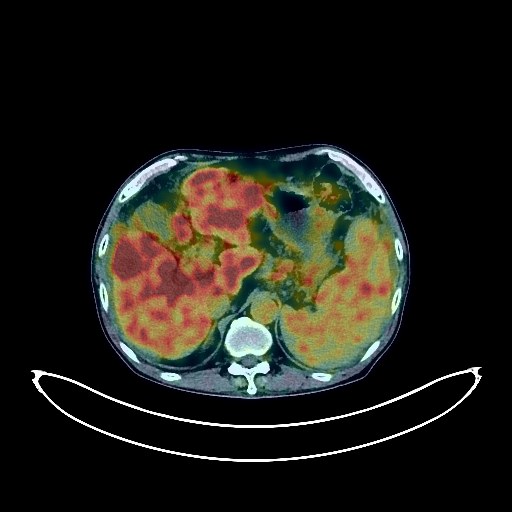
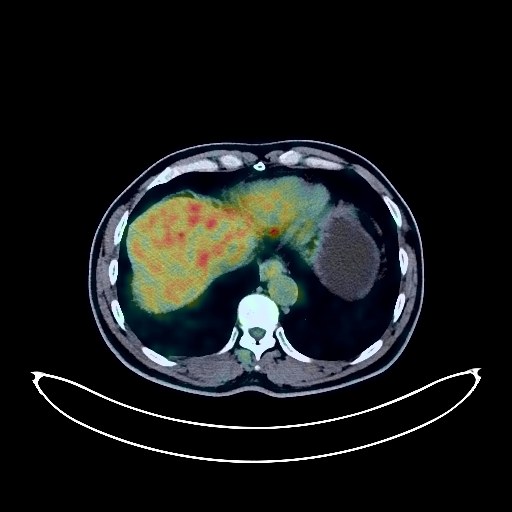
Liver Cancer PET/CT (case 983827-000194 from PETWB-REP)
0 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Liver Cancer taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression a. Multiple intrahepatic lesions with increased FDG metabolism, suggestive of hepatocellular carcinoma with multiple intrahepatic lesions; please correlate with clinicopathology. b. Multiple lymph node metastases in the portal vena cava space and retroperitoneum. Multiple bone metastases throughout the body. Left inferior deep cervical lymph node metastasis to be ruled out. c. Cirrhosis, splenomegaly, portal hypertension, esophageal and gastric varices. Accessory spleens (multiple). d. Abdominal and pelvic effusion. Increased density and blurred appearance of the abdominal fat space and mesentery, with slightly increased FDG uptake, suggestive of panniculitis; metastasis cannot be ruled out. Mixed ground-glass nodules in the apical-posterior segment of the left upper lobe, with normal FDG uptake, highly suggestive of inflammatory lesions; CT scan recommended for comparison to rule out tumors. Multiple small chronic inflammatory nodules in both lungs; CT follow-up recommended. Chronic bronchitis in both lungs. Scattered post-inflammatory lesions in both lungs. Reactive hyperplasia of the left hilar lymph nodes. Calcification of the mediastinal and bilateral hilar lymph nodes. Sclerosis of the aorta and its branches. Bilateral breast development. Slight thickening of the esophageal cardia and part of the gastric wall; FDG metabolism normal, suggestive of gastritis. Physiological uptake of part of the intestine. Chronic cholecystitis. Left renal cyst. Prostatic calcification. Calcification in the right lobe of the thyroid gland; please combine with ultrasound examination. Degenerative changes in the spine. L3/4 and L4/5 intervertebral disc bulge. L5/S1 intervertebral disc herniation. Senile brain; a few lacunar ischemic lesions deep in the brain. Chronic inflammation of the left maxillary sinus and left sphenoid sinus. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT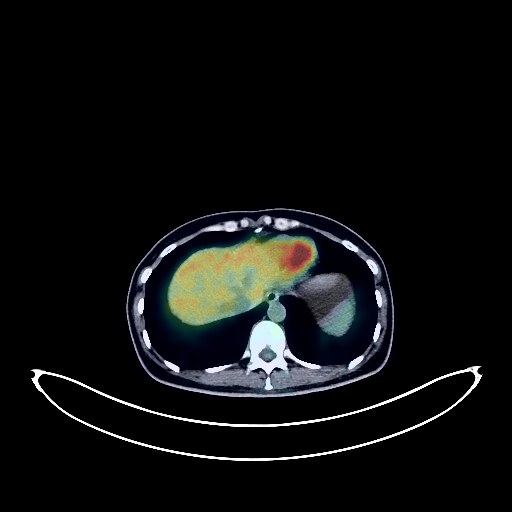
Colon Cancer PET/CT (case 983827-000072 from PETWB-REP)
0 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Colon Cancer taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression a. No obvious signs of tumor recurrence were observed after comprehensive treatment for colon cancer. b. A cystic mass in the retroperitoneum of the mid-abdomen, with no obvious abnormalities in FDG uptake, is considered a possible cyst. Further MRI with contrast is recommended to rule out other possibilities. Multiple ground-glass nodules in the left upper lobe and right lower lobe, with no abnormalities in FDG metabolism, are considered atypical adenomatous hyperplasia or inflammatory nodules. Annual HRCT follow-up is recommended. Mild osteophyte formation in the spine. Subcutaneous calcifications in both buttocks. Left temporal meningioma, MRI with contrast is recommended for follow-up. A slightly low-density nodule in liver S5 shown on CT scan at another hospital was not clearly visualized in this examination. Further MRI with contrast is recommended. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT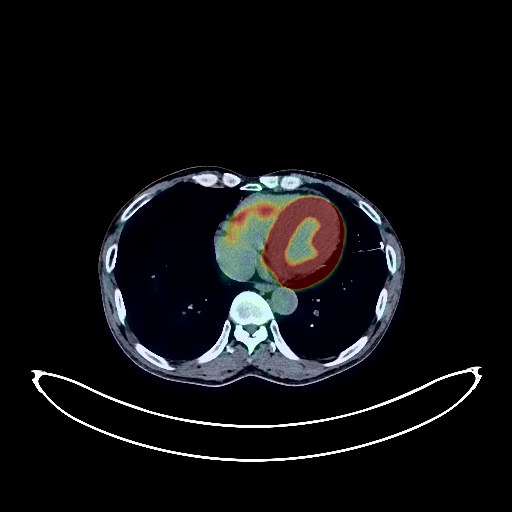
Colon Cancer PET/CT (case 983827-000222 from PETWB-REP)
0 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Colon Cancer taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression Irregular thickening of the descending colon wall with increased FDG metabolism suggests colorectal cancer. Irregular thickening of the ascending colon wall near the hepatic flexure with increased FDG metabolism also suggests colorectal cancer. a. Old lesions in the apical segment of the right upper lobe and the posterior segment of the left lower lobe. Chronic inflammatory micronodules in both lungs. Emphysema in both lungs, scattered post-inflammatory remnants in both lungs. b. Reactive hyperplasia of mediastinal lymph nodes. Pleural thickening bilaterally, with calcification on the left. Calcification of some arterial walls (including coronary arteries). Small liver cysts. Cystic mass in the tail of the pancreas, likely a cyst, cystadenoma to be ruled out; enhanced MRI follow-up recommended. Left cryptorchidism. Chronic inflammatory changes in part of the gastric wall; please follow up with endoscopy. Hemorrhoidal changes. Degenerative changes in the spine, postoperative changes after lumbar spine surgery. Bilateral frozen shoulder. No obvious abnormalities were found on cranial scintigraphy. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT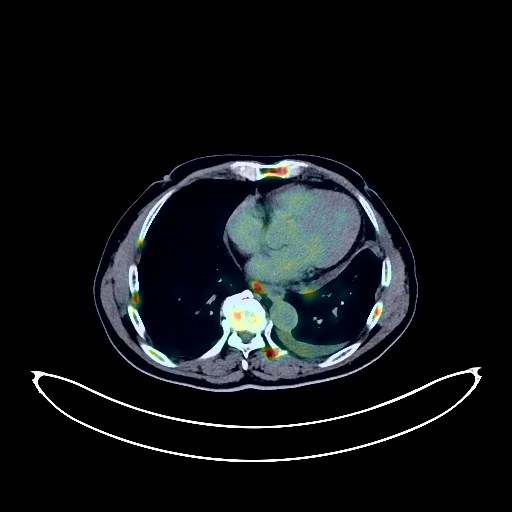
Lung Cancer PET/CT (case 983827-000022 from PETWB-REP)
0 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Lung Cancer taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression a. A mass near the hilum of the left upper lobe, with increased FDG metabolism, suggestive of central lung cancer. Multiple lymph node metastases in the right submandibular region, right supraclavicular fossa, left hilum, mediastinum, peripancreatic region, and retroperitoneum. Bilateral adrenal metastases. Multiple liver metastases. Multiple bone metastases throughout the body (pathological fractures of some ribs on the right side). b. Small amount of pleural effusion on the left side. Small amount of pericardial effusion. Calcification of some arterial walls (including coronary arteries). c. A few chronic inflammatory lesions and old lesions in both lungs. Accessory spleen. A few calcifications in the prostate. Degenerative changes in the spine. L4/5 and L5/S1 intervertebral disc bulges. Intracerebral ischemic lesions, age-related brain changes; follow-up MRI is recommended. Submucosal cyst of the left maxillary sinus. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT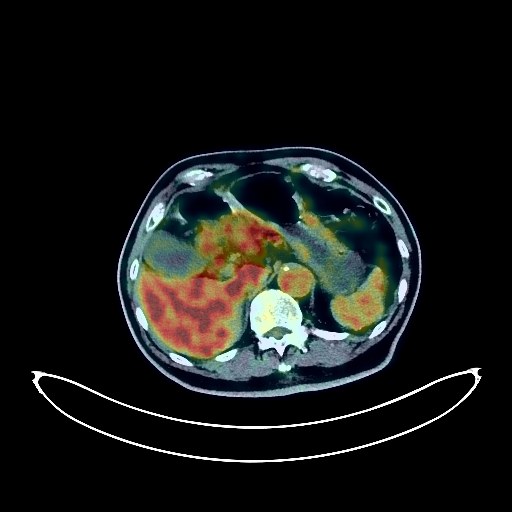
Pancreatic Cancer PET/CT (case 983827-000013 from PETWB-REP)
0 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Pancreatic Cancer taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression a. Massive lesions in the body and tail of the pancreas with elevated FDG metabolism, suggestive of pancreatic cancer with peripancreatic lymph node metastasis. Please combine tumor markers and enhanced MRI for comprehensive analysis. b. Peritoneal seeding metastasis; small amount of pelvic effusion. a. Chronic inflammatory nodules in both lungs. Interstitial changes in both lungs, emphysema with bullae in both lungs, old pulmonary tuberculosis in both lungs. Pleural thickening bilaterally. Chronic inflammatory lymph nodes in the hilum and mediastinum of both lungs. Calcification of some arterial walls (including coronary arteries). b. Low-density nodule in the anterior mediastinum, no abnormalities in FDG metabolism, suggestive of benign nodule, follow-up is recommended. Cyst and calcification in the right lobe of the liver. Hyperplasia of the left adrenal gland. Multiple cysts in the left kidney. Prostatic hyperplasia with calcification. Chronic inflammatory changes in the cardia, antrum of the stomach, and part of the intestine. Please follow up with endoscopy. Osteoporosis, degenerative changes in the spine, L4/5 and L5/S1 disc bulges. L4/5 disc degeneration with pneumoconiosis. Age-related brain conditions, deep lacunar infarcts. Chronic inflammation of the right lateral nasopharyngeal wall. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT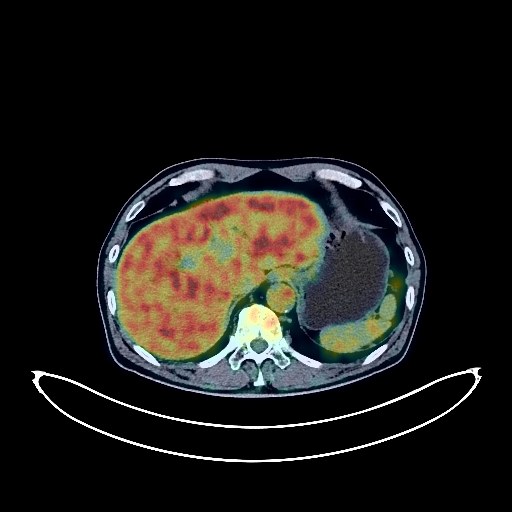
Pancreatic Cancer PET/CT (case 983827-000160 from PETWB-REP)
0 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Pancreatic Cancer taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression a. A soft tissue mass in the head of the pancreas with dilation of the upstream pancreatic duct and biliary system, and increased FDG metabolism, suggestive of pancreatic cancer. b. Multiple solid nodules in both lungs, most likely chronic inflammatory nodules, with the larger one in the posterior segment of the left lower lobe showing increased FDG metabolism; metastasis cannot be ruled out. Please follow up with CT scans. c. Small lymph nodes in the hepatogastric space, porta hepatis, and retroperitoneum are present, but FDG metabolism is not increased, suggesting reactive lymph node hyperplasia. Please follow up with CT scans to rule out other complications. A mass on the left posterolateral wall of the bladder, most likely a bladder tumor. Please conduct further examination with enhanced CT or cystoscopy. Bilateral adrenal adenomas. Right renal cyst. Prostatic calcifications. Enlarged gallbladder with cholestasis. Small amount of pelvic effusion. Manifestations of chronic gastritis, with physiological uptake of the small intestine in the right mid-abdomen. Calcified nodules in the anterior wall of the gastric fundus; gastroscopy and enhanced CT scans may be necessary. Bilateral emphysema, interstitial lung changes, a few chronic inflammations and sequelae in both lungs. Tracheal diverticulum. Reactive hyperplasia of bilateral hilar and mediastinal lymph nodes. Partial arteriosclerosis (including coronary arteries). Degenerative changes in the spine, L3/4 disc bulge, slight L4/5 disc protrusion. Sebaceous cyst in the right shoulder. Left upper periodontitis. Reactive hyperplasia of bilateral superior deep cervical lymph nodes. Deep lacunar infarcts in the brain. A few chronic inflammations in the right sphenoid sinus and left maxillary sinus. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT