Loading...
Breast Cancer PET/CT (case 983824-000026 from PETWB-REP)
9 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Breast Cancer taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression a. A mass in the upper inner quadrant of the left breast with increased FDG metabolism, suggestive of breast cancer; bilateral breast hyperplasia; b. Multiple lymph node metastases in the left axilla, left pectoral intermuscular space, left supraclavicular fossa, left posterior cervical triangle, and left deep cervical space; liver metastases; c. Small nodular FDG-enhanced foci in the lateral part of the left breast, suggestive of breast cancer, please correlate with clinical findings. a. Ground-glass nodules in the upper lobes of both lungs and the posterior basal segment of the left lower lobe, with normal FDG metabolism, suggestive of inflammation or atypical adenomatous hyperplasia, CT follow-up recommended; b. Chronic inflammatory nodule in the upper lobe of the right lung, CT follow-up recommended. A few post-inflammatory lesions in both lungs. Reactive hyperplasia of mediastinal lymph nodes. Chronic cholecystitis. Intrauterine device insertion, uterine fibroids are highly likely, please correlate with ultrasound examination. Chronic inflammatory changes or physiological uptake in part of the gastric wall and intestinal tract, please correlate with endoscopy. L4/5 intervertebral disc bulge. Subcutaneous calcifications in the left buttock. Uneven thyroid density with diffusely increased FDG metabolism in the lobes, suggesting possible inflammation; please confirm with ultrasound and laboratory tests. No obvious abnormalities seen on cranial scintigraphy. Chronic inflammation of the left nasopharyngeal wall. Chronic inflammation of both ethmoid sinuses and the left maxillary sinus. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT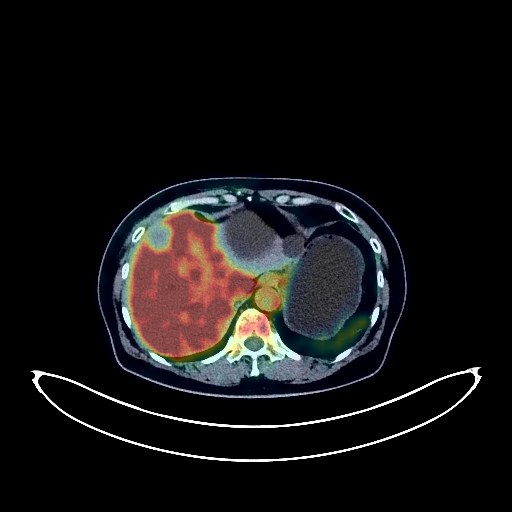
Breast Cancer PET/CT (case 983824-000032 from PETWB-REP)
8 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Breast Cancer taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression a. Thickened skin of the right breast, mass in the lower inner quadrant of the right breast, increased FDG metabolism, suggestive of breast cancer; please refer to pathology. Calcifications in the right breast. b. Lymph node metastasis in the right axilla and right internal mammary chain. Ground-glass nodules in the apical segment of the right upper lobe and the lateral basal segment of the right lower lobe, normal FDG metabolism, suggestive of chronic inflammatory nodules or atypical adenomatous hyperplasia; please refer to annual follow-up with HRCT. Chronic inflammation and sequelae in both lungs. Liver cyst (one large). Left kidney cyst. Uterine fibroid. Increased FDG metabolism in some intestinal segments, suggestive of physiological uptake or chronic inflammation; please refer to endoscopic follow-up. Spinal degeneration. Inflammation of the L5/S1 facet joint. L4/5 intervertebral disc bulge, pneumatosis, and degeneration. Bilateral deep lacunar infarcts, senile encephalopathy. Bilateral ethmoid sinusitis. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT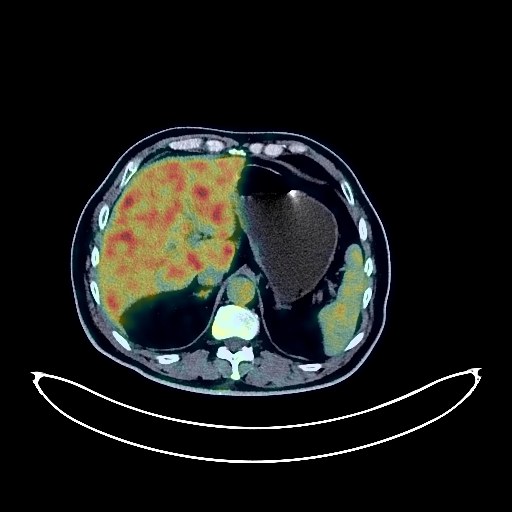
Lung Cancer PET/CT (case 983824-000082 from PETWB-REP)
7 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Lung Cancer taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression a. A mass in the posterior segment of the right lower lobe, with increased FDG metabolism, suggestive of lung cancer with obstructive changes; please correlate with clinicopathology. b. Small to moderate pleural effusion on the right side. Slight pleural thickening bilaterally. Possible reactive hyperplasia of hilar and mediastinal lymph nodes, with partial metastasis to be ruled out; follow-up is recommended. c. Several small, solid, chronic inflammatory nodules in both lungs. Partial bronchiectasis in both lungs. Scattered chronic inflammation and old lesions in both lungs. Calcification of some arterial walls (including coronary arteries). Calcification in the liver. Bilateral renal cysts. Benign prostatic hyperplasia with calcification. Enlargement of the right inguinal canal. Mild posterior slippage of the L2 and L3 vertebral bodies. Degenerative changes in the spine. L4/5 and L5/S1 intervertebral disc bulges. A few ischemic lesions in the deep bilateral brain regions; age-related brain. Follow-up MRI is recommended. Enlarged thyroid gland with uneven density; FDG uptake normal; nodular goiter suggested; ultrasound examination recommended. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT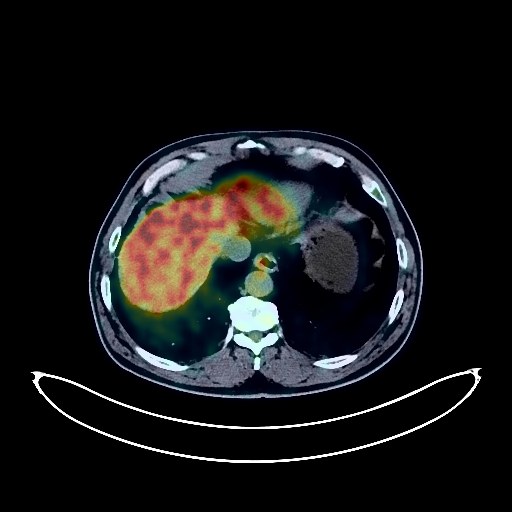
Renal Cancer PET/CT (case 983824-000110 from PETWB-REP)
4 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Renal Cancer taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression a. Post-right renal cell carcinoma surgery, changes observed in the right kidney, multiple lesions in both kidneys with increased FDG metabolism, suggestive of malignancy; please correlate with clinical findings and enhanced MRI for diagnosis; left renal calculi. b. Multiple solid nodules in both lungs, well-defined borders, some with slightly increased FDG metabolism, suggestive of chronic inflammatory nodules; metastasis of some larger nodules (posterior basal segment of the left lower lobe) cannot be ruled out; CT follow-up observation is recommended. c. Enlarged subcarinal lymph nodes with increased FDG metabolism, suggestive of metastasis; please correlate with clinical findings. Chronic inflammation and post-inflammatory remnants in both lungs; CT follow-up is recommended. Partial arteriosclerosis. Gallbladder: concentrated bile or residual contrast agent. Prostatic calcification. Reactive hyperplasia of retroperitoneal lymph nodes. Chronic inflammatory changes in part of the gastric wall, hemorrhoidal changes; please follow up with endoscopy. Degenerative changes in the spine, L3/4, L4/5, L5/S1 intervertebral disc bulge. Left sacral islet. Bilateral acromioclavicular joint inflammation. Widened septum pellucidum, no obvious abnormalities seen on cranial scintigraphy. Bilateral chronic ethmoid sinusitis. Inflammation of the right lateral oropharyngeal wall, base of the tongue, and bilateral palatine tonsils. Reactive hyperplasia of right cervical lymph nodes. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT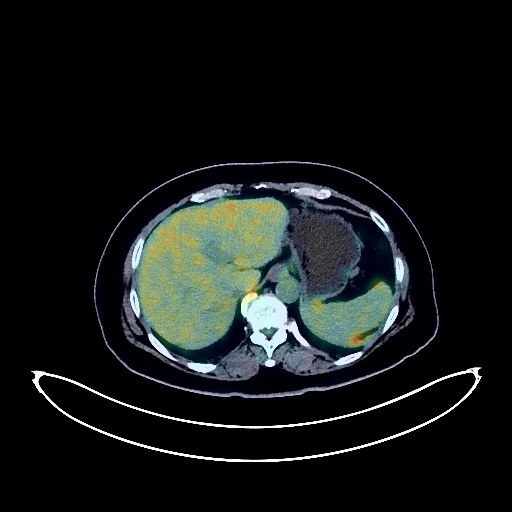
Pancreatic Cancer PET/CT (case 983824-000092 from PETWB-REP)
4 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Pancreatic Cancer taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression a. A mass in the pancreatic body with increased FDG metabolism, suggestive of pancreatic cancer, with invasion of splenic vessels. b. Extensive peritoneal seeding metastases in the abdominopelvic cavity. c. Mesenteric panniculitis. Several small, solid, chronic inflammatory nodules in both lungs. A few chronic inflammatory lesions and old lesions in both lungs. Calcification of some arterial walls (including coronary arteries). A complex small cyst in the left kidney. Degenerative changes in the spine. L4/5 and L5/S1 intervertebral disc herniation with pneumoconiosis and degeneration. Bilateral acromioclavicular arthritis. A few ischemic lesions in the deep bilateral brain regions. Small lipoma in the midline of the brain. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT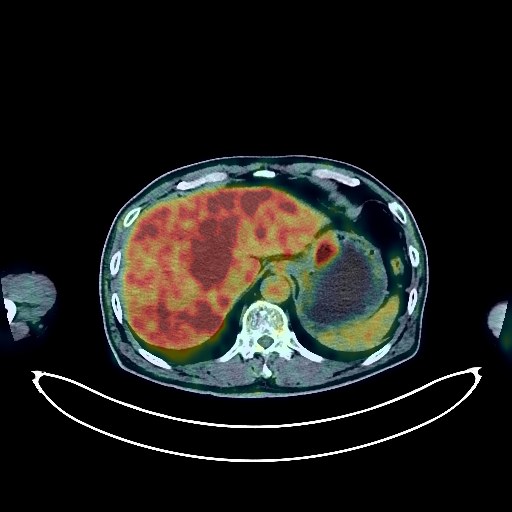
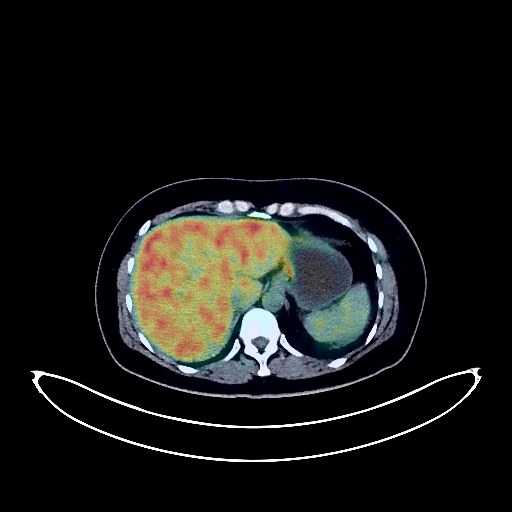
Liver Cancer PET/CT (case 983824-000164 from PETWB-REP)
4 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Liver Cancer taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression a. Multiple space-occupying lesions in the liver with elevated FDG metabolism, suggestive of malignancy, with a high probability of metastasis. Primary intrahepatic tumor with intrahepatic metastasis needs further investigation. Please combine tumor markers and enhanced MRI for comprehensive analysis. Metastasis to the hilar lymph nodes, hepatogastric space, and pancreatic head. b. Thickening of the gastric wall on the lesser curvature of the gastric body with elevated FDG metabolism, suggestive of gastric cancer. Further gastroscopy is recommended. a. Ground-glass nodule in the apical segment of the right upper lobe, with normal FDG metabolism, suggestive of inflammation or atypical adenomatous hyperplasia. Follow-up is recommended. b. Chronic inflammatory micronodules (solid) in both lungs. Mild emphysema in the upper lobes of both lungs. Scattered post-inflammatory lesions in both lungs. Anemia changes, partial arterial wall calcification (including coronary arteries). Small cyst in the left kidney. Calcification lesions in the prostate. Degenerative changes in the spine, L3/4 and L4/5 disc bulge. Bilateral frozen shoulder. Cranial scintigraphy showed no obvious abnormalities. Minor chronic inflammation of the right ethmoid and maxillary sinuses. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT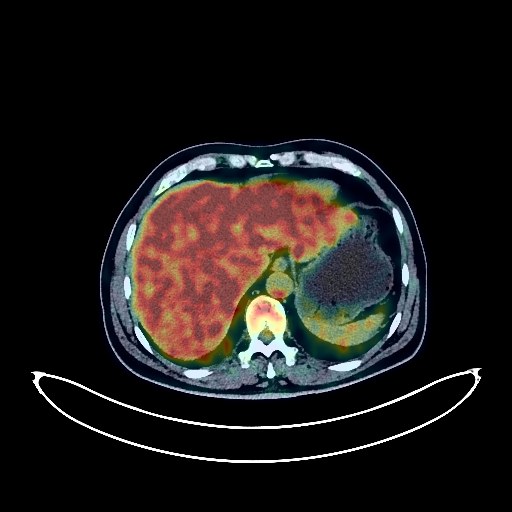
Lung Cancer PET/CT (case 983824-000150 from PETWB-REP)
4 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Lung Cancer taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression a. Left hilar mass, elevated FDG metabolism, suggestive of central lung cancer with obstructive inflammation or atelectasis; please confirm with pathological examination. b. Left hilar lymph node metastasis. Highly likely reactive hyperplasia of mediastinal and right hilar lymph nodes; follow-up recommended. c. Bilateral chronic inflammatory micronodules; follow-up recommended. Scattered chronic inflammation and remnants in both lungs. Subpleural bullae in the posterior segment of the right lower lobe. Slight pleural thickening bilaterally. Localized thickening of the sigmoid colon and rectum, elevated FDG metabolism, suggestive of inflammatory polyps; colonoscopy recommended to rule out tumors. Possible cholestasis; ultrasound follow-up recommended. Reactive hyperplasia of small retroperitoneal lymph nodes. Degenerative changes in the spine. Lumbar vertebral endplate inflammation. L4/5 disc bulge. L5/S1 disc herniation. Left hip periarthritis. Few ischemic lesions in the deep bilateral brain; age-related brain, MRI recommended. Slight chronic inflammation of the right maxillary sinus. Reactive hyperplasia of bilateral submandibular lymph nodes. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT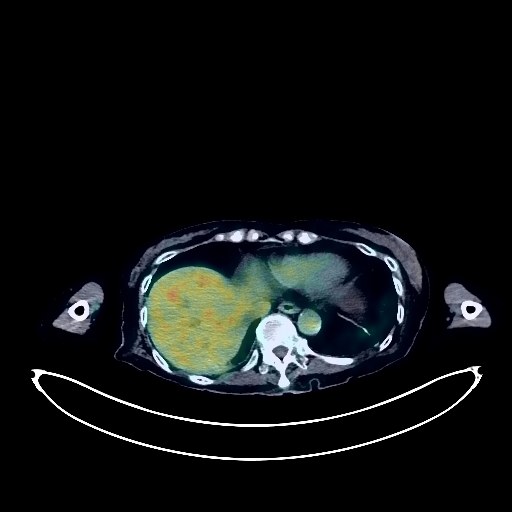
Cholangiocarcinoma PET/CT (case 983824-000047 from PETWB-REP)
10 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Cholangiocarcinoma taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression a. Post-PTCD, increased FDG uptake along the indwelling catheter suggests possible post-operative changes, but local tumor uptake cannot be ruled out; no clear space-occupying lesion was seen in the common bile duct area, but intrahepatic bile duct dilation was observed. The above findings should be analyzed in conjunction with enhanced MRI images. b. A metastatic tumor in the left pubic tubercle is highly probable; follow-up is recommended. Reactive hyperplasia of small lymph nodes in the retroperitoneum and bilateral iliac vessels is observed. c. Gallstones or calcifications in the gallbladder, chronic cholecystitis, without clear space-occupying lesions. Uneven density between the left and right lobes of the thyroid gland; slight enlargement of the right thyroid lobe with slightly low-density nodules, increased FDG metabolism, suggesting adenoma; malignancy needs to be ruled out. Further ultrasound examination is recommended, with biopsy if necessary. a. Ground-glass opacity in the apical segment of the right upper lobe, with normal FDG metabolism, suggests chronic inflammatory changes or atypical adenomatous hyperplasia. A follow-up HRCT scan every six months is recommended. b. Chronic inflammatory nodules and nodular lesions in both lungs. A few chronic inflammatory lesions and sequelae in both lungs. Slight thickening of the pleura on both sides, with a small amount of pleural effusion in both pleural cavities. Calcification of some arterial walls (including coronary arteries). Cystic lesions in the neck of the pancreas. Left adrenal hyperplasia. Calcification of the uterus. Slight thickening of the gastric antrum wall with increased FDG metabolism, and increased FDG metabolism in some intestinal segments, suggestive of chronic inflammatory changes or physiological uptake. Osteoporosis, scoliosis with degenerative changes, Schmorl's nodes in the T12 and L2 vertebral bodies. Intervertebral disc bulges at L3/4, L4/5, and L5/S1. Left hip periarthritis. Left sacral wing fracture due to failure. Bilateral deep cerebral ischemic lesions, age-related brain changes. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT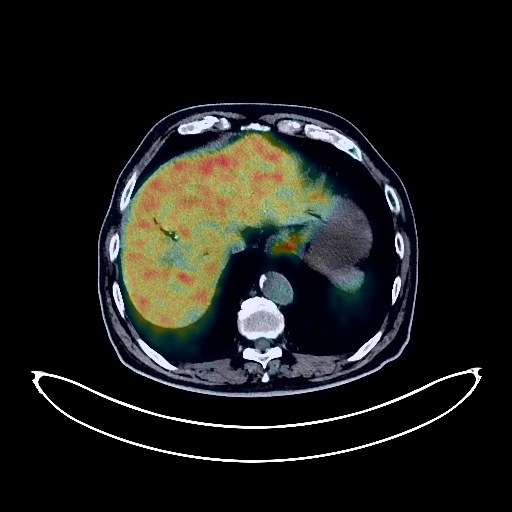
Pancreatic Cancer PET/CT (case 983824-000212 from PETWB-REP)
4 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Pancreatic Cancer taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression a. An irregular soft tissue mass in the head of the pancreas, with increased FDG metabolism, suggests a malignant tumor, possibly pancreatic cancer, but metastasis cannot be ruled out. The boundary with adjacent blood vessels is unclear. Metastasis is present in the hepatogastric space, retroperitoneal para-aortic lymph nodes, mesenteric space, and para-aortic lymph nodes. b. Post-choledochal stent placement, increased FDG metabolism in the bile ducts surrounding the upper end of the stent in the porta hepatis suggests possible inflammatory changes, with neoplastic lesions to be ruled out. Intrahepatic bile duct dilation and pneumoconiosis are present. The gallbladder is not clearly visualized. Pelvic effusion is present. Please combine the above with tumor markers, enhanced MRI, and MRCP for comprehensive analysis. A mass in the cardia, it is recommended to combine with the pathology report of an external gastroscopy; chronic inflammation of the gastric antrum. Discontinuous esophageal FDG metabolism is present, but physiological uptake should be considered in conjunction with an external gastroscopy report. 3.a. Pure ground-glass nodules in the left upper lobe and right lower lobe, with normal FDG metabolism, suggestive of chronic inflammatory nodules or atypical adenomatous hyperplasia. Please combine with annual HRCT follow-up. b. Chronic inflammatory micronodules (solid) in both lungs, paraseptal emphysema in both upper lobes, please combine with CT follow-up. Reactive hyperplasia of hilar and mediastinal lymph nodes in both lungs. Partial arteriosclerosis (including coronary arteries). Right kidney stone, bilateral ureteral stones. Prostatic calcification, please combine with PSA follow-up. Bilateral adrenal hyperplasia is highly probable. Increased FDG metabolism in some intestinal segments, suggestive of physiological uptake or chronic inflammation, hemorrhoidal changes, please combine with endoscopy follow-up. Spinal degenerative changes. Mild anterior slippage of L4 vertebral body. L2-S1 intervertebral disc bulge, with partial pneumothorax and degeneration of the thoracolumbar intervertebral discs. Bilateral deep lacunar infarcts, age-related brain changes. Low-density thyroid nodules, with increased FDG metabolism at the margins of some nodules, suggesting possible nodular goiter; ultrasound follow-up is recommended. Reactive hyperplasia of cervical lymph nodes. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT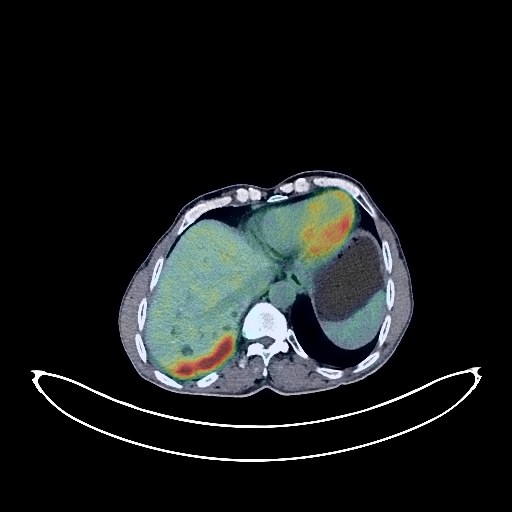
Lung Cancer PET/CT (case 983824-000028 from PETWB-REP)
11 views10 days agoWhole-body 18F-FDG PET/CT scan in a patient with Lung Cancer taken from the PETWB-REP dataset. The following English report (translated from original Chinese) is taken verbatim from the public dataset and has not been modified or otherwise checked for accuracy (see the end for citation). Impression a. A mass in the lower lobe of the right lung, with elevated FDG metabolism, suggestive of lung cancer with obstructive changes. Bilateral lung metastases. Extensive metastasis to the right interlobar pleura. Small amount of pleural effusion on the right side. b. Metastasis to lymph nodes in the right hilum and mediastinum. Possible metastasis to the right anterior diaphragmatic lymph nodes. c. Scattered chronic inflammation and old lesions in both lungs. Asymmetrical chest wall. Calcification of some arterial walls. Multiple cysts in the liver. Contrast agent residue in the gallbladder. Bilateral renal cysts, calcification in the left kidney. Mild anterior slippage of the L4 vertebral body. Scoliosis. Degenerative changes in the spine. L4/5 and L5/S1 intervertebral disc bulges. A few ischemic lesions in the deep bilateral brain regions, age-related brain changes. This case is from PETWB-REP, a curated dataset of whole-body 18F-FDG PET/CT scans and corresponding radiology reports from 490 patients with a broad spectrum of malignancies. The data were retrospectively collected from patients who underwent clinically indicated whole-body 18F-FDG PET/CT scans at the Shanghai Universal Medical Imaging Diagnostic Center between 2021 and 2024. License: Creative Commons Attribution 4.0 International (CC BY 4.0) Citation: Xue, L., Feng, G., Wenbo, Z., Zhang, Y., Li, L., Wang, S., Peng, L., Peng, S., & Gao, X. (2026). PETWB-REP: A Multi-Cancer Whole-Body FDG PET/CT Dataset with Corresponding Radiology Reports [Data set]. Zenodo. https://doi.org/10.5281/zenodo.18670487
Whole BodyPET/CT