Loading...
EDNeuroRad Cases
94 cases
Updated 7 months ago
EEDNeuroRad
A comprehensive collection of cases from the website EDNeuroRad.com covering various emergent and urgent neuroradiology conditions. Great for call preparation as a resident.

Cortical contusions and subarachnoid hemorrhage (EDNeurorad Case 1)
695 views
8 months ago
Near the vertex, there are superficial hyperdensities along/within the cortex on both sides (@Key Finding 1). Some as pointed to by the red arrow truly appear to be within the cortex and are therefore small areas of cortical contusion. Others such as pointed to by the green arrow are located within a sulcus (best seen on the sagital reformation from the thins @Key Finding 2) and are therefore consistent with areas of subarachnoid hemorrhage.
Head
CT
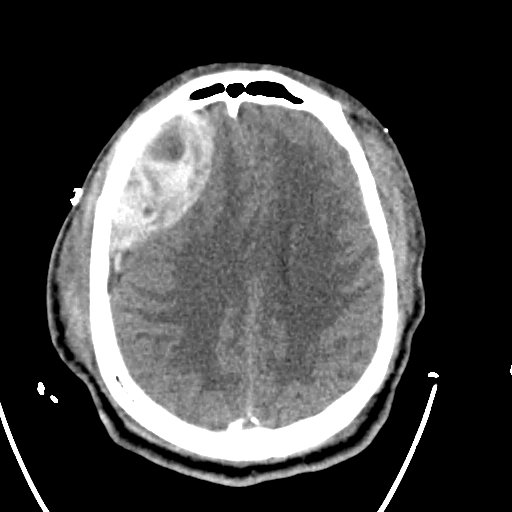
Skull fracture, epidural hematoma, orbital hematoma (EDNeurorad Case 2)
333 views
9 months ago
There is a lentiform shaped large right anterior frontoparietal convexity extra-axial hematoma @Key Finding 1. Clearly, the shape of the hematoma suggests that it is epidural in location but it does cross the coronal suture @Key Finding 2, something that epidural hematomas should not do due to the tight dural adhesion at the sutures. Here, there is a parietal bone fracture that clearly extends to the coronal suture and so the dural attachments are likely disrupted allowing for the hematoma to cross the suture. Epidural location of this hematoma was surgically confirmed.There are areas of parenchymal contusion both in the right inferior frontal lobe and the high right fronto-parietal lobe near the vertex (@Key Finding 3, @Key Finding 4).Note in addition that the right parietal bone fracture extends inferiorly to the greater wing of the right sphenoid bone as well as the superolateral orbital wall (@Key Finding 6). There is an associated intra-orbital, extra-conal hematoma exerting mass effect upon the right lateral rectus muscle (@Key Finding 5).Finally, notice that the sphenoid sinuses both have layering hematocrit levels. There is a fracture of the left sphenoid sinus lateral wall as well as a fracture of the sphenoid septum (@Key Finding 7).Incidentally, the patient had already undergone a right frontal burr hole for placement of an intracranial pressure monitoring device prior to this head CT. The outside hospital imaging prior to this head CT did not demonstrate the epidural hematoma.
Head
CT

Subdural hematoma (EDNeurorad Case 3a)
207 views
8 months ago
There is a predominantly hyperdense left cerebral convexity subdural hematoma (@Key Finding 1). Near the vertex, there is a layering hematocrit level, typically seen in the setting of either active bleeding or coagulopathy (@Key Finding 2). The hematoma results in mass effect as evidenced by effacement of the left lateral ventricle compared to the right and midline shift.As nicely seen on the coronal reformations from the thin section data (@Key Finding 3), the hematoma has components along the left tentorium (red arrow) and the falx (green arrow). These can also be seen on the axial images.
Head
CT

Right subdural hematoma (EDNeurorad Case 3b)
172 views
8 months ago
Clearly, there are post surgical changes from left subdural hematoma evacuation with a subdural drainage catheter in place (@Key Finding 1). However, there is now a lentiform extra-axial hematoma over the right parietal convexity, particularly evident on the coronal reformation (@Key Finding 2). The hematoma does not cross any sutures, although it is not large enough to approach the sutures yet. These imaging features are those of an epidural hematoma. The only odd aspect of this case is that there was no new trauma to cause an epidural hematoma. The hematoma was surgically confirmed to be in the subdural space so this is a great mimic case and an illustration that nothing is 100% accurate in imaging!Notice the additional subdural hematomas (@Key Finding 3) along the falx (green arrow), left tentorium (red arrow), and the right posterior fossa (red arrowhead).
Head
CT
Subacute subdural hematomas (EDNeurorad Case 4)
154 views
8 months ago
There are bilateral iso-attenuating subdural hematomas , consistent with a subacute time course (@Key Finding 1). The hematoma on the right has areas of hyperattenuation and is likely an acute on subacute hematoma. These are sizable hematomas, with some hyperattenuation on the right so they are relatively obvious to detect. For trickier cases, you need to pay careful attention to the cortex and notice areas of asymmetric apparent thickening and displacement, as seen here for the left sided hematoma.
Head
CT

Subtle subdural hematoma (EDNeurorad Case 5)
157 views
8 months ago
There is a very small left convexity subdural hematoma, seen on multiple continuous slices (@Key Finding 1, @Key Finding 2). The best chance to catch this would be to use subdural windows (here I used width of roughly 150 and center of 80). The hematoma increased in conspicuity on subsequent head CTs.
Head
CT
Intraparenchymal and subarachnoid hemorrhage (EDNeurorad Case 6)
164 views
8 months ago
There is a small intraparenchymal hematoma with adjacent vasogenic edema in the right frontal lobe (red arrow, @Key Finding 1). Additional subarachnoid hemorrhage is seen in the adjacent frontal sulci (green arrows, @Key Finding 2). The etiology in this case is unclear.
Head
CT
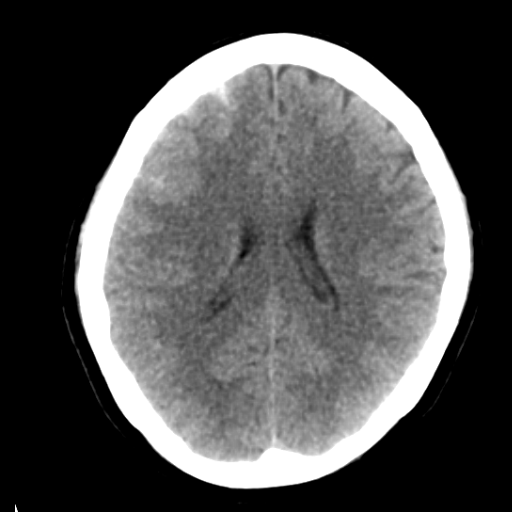
Hypoxic ischemic injury (EDNeurorad Case 7)
174 views
8 months ago
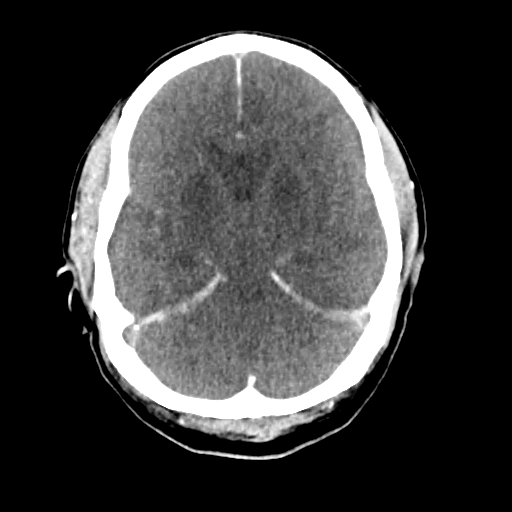
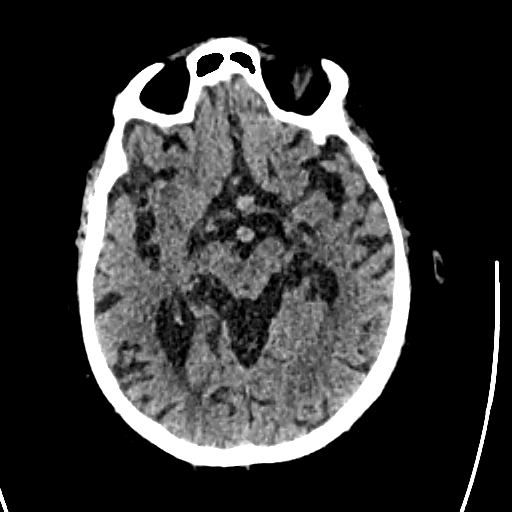
There is hypoattenuation in the basal ganglia and thalami with loss of the normal gray-white differentiation (red outline, @Key Finding 1). There are findings of diffuse cerebral edema with effacement of all basilar cisterns, cerebral sulci, and the ventricles. In addition, there is a "pseudo-subarachnoid" hemorrhage appearance (green arrows) caused by the edematous and hypodense brain being in close apposition to the normal MCA and ACA branches which appear hyperdense. Notice also how hyperdense the dura (e.g. falx, tentoria) appear compared to the edematous brain. These are all findings of profound hypoxic ischemic injury.
Head
CT
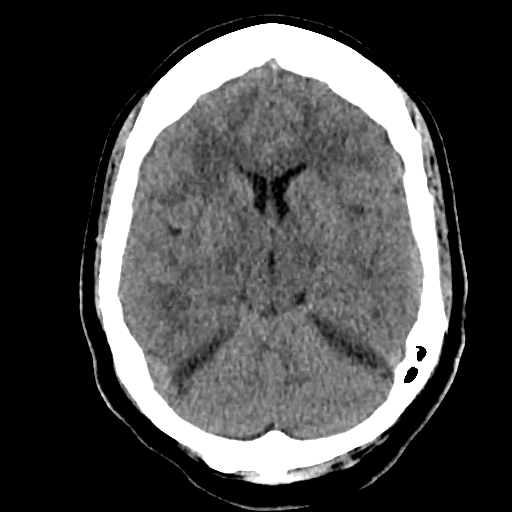
Right MCA stroke (EDNeurorad Case 8a)
164 views
8 months ago
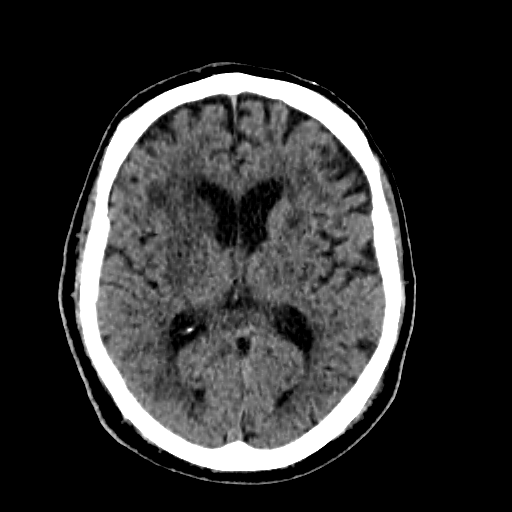
When comparing the right basal ganglia to the left (@Key Finding 1, red outlined area compared to green outlined area), you will notice subtle hypoattenuation with loss of gray-white differentiation. This is typical of an acute infarct within the right MCA territory
Head
CT
Right M1 occlusion (EDNeurorad Case 8b)
119 views
8 months ago
@Key Finding 1 shows abrupt loss of opacification in the M1 segment of the right MCA. On @Key Finding 2 we see associated geographic paucity of vascular opacification in the distal right MCA branches.
Head and neck
CTA

Hyperdense right M2 (EDNeurorad Case 9a)
160 views
8 months ago
There is a very prominent hyperdense right M2 branch within the sylvian fissure (red arrow, @Key Finding 1). The vascular nature of this can be confirmed by looking at the adjacent slices, particularly on the thin sections. This is suspicious for a thromus within an M2 branch of the MCA.
Head
CT
Right M2 occlusion with right MCA infarct (EDNeurorad Case 9b)
136 views
8 months ago
There is a perfusion defect in the right parietal lobe with a wedge shaped area of elevated TMAX (@Key Finding 1), diminished CBF (@Key Finding 2), and relatively preserved CBV (@Key Finding 3). This pattern would typically be expected with an infarct that has salvagable tissue and not much infarct core.There is an associated right M2 branch occlusion with the occlusion at slice 367-368/510 on the CTA (@Key Finding 4). This matches nicely the location of the hyperdense M2 on the non-con head CT from Case 9a.As a bonus, did you catch the incidental mass in the deep lobe of the left parotid gland (@Key Finding 5)? It turned out to be a Warthin tumor.
Head and Neck
CTA, CTP
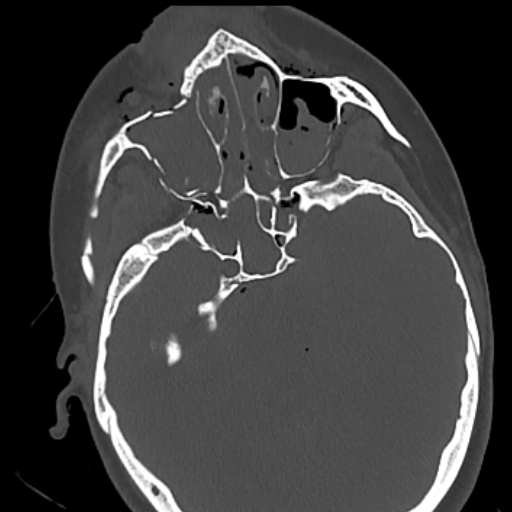
Right cerebellar infarct, clival meningioma (EDNeurorad Case 10)
139 views
8 months ago
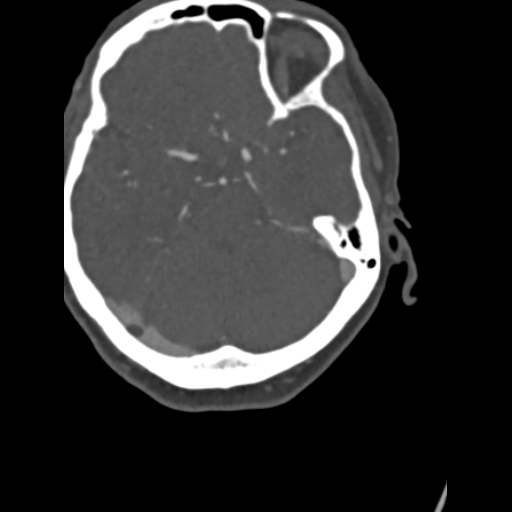
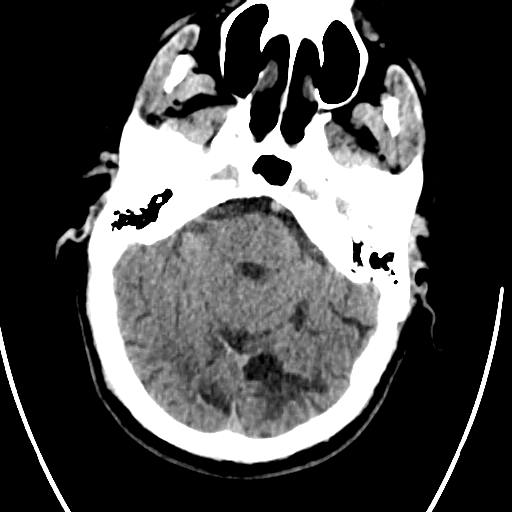
There is a wedge-shaped area of hypoattenuation with loss of gray-white differentiation in the right cerebellum consistent with an acute or early subacute infarct (@Key Finding 1). ---The much bigger finding, and surprisingly much more challenging to see due to the poor head positioning, is the large retroclival extra-axial mass that's compressing the medulla and pons (@Key Finding 2, @Key Finding 3)!
Head
CT
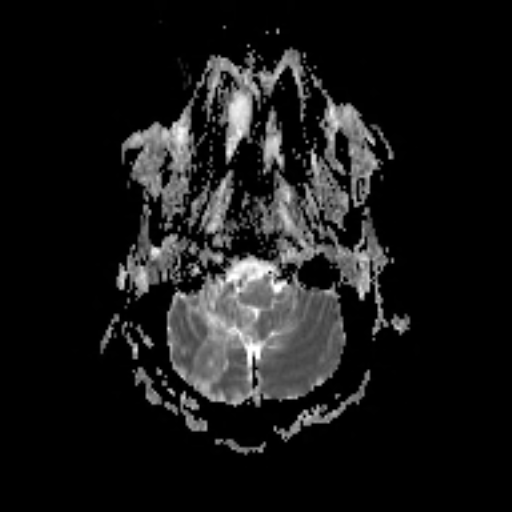
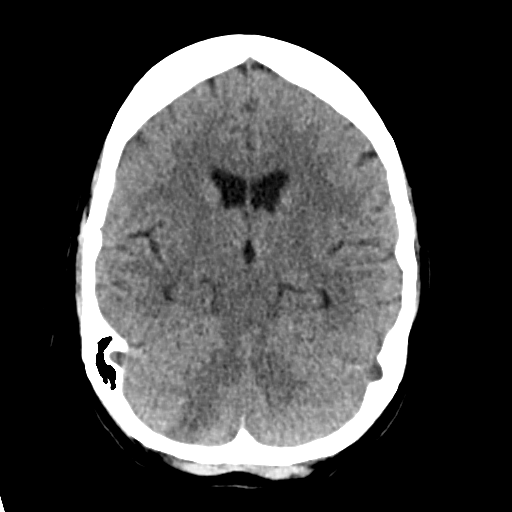
Retroclival meningioma with subacute right PICA territory infarct (EDNeurorad Case 11)
155 views
8 months ago
The infarct is subacute in its timecourse: It has already pseudo-normalized on ADC (@Key Finding 1), has small areas of pre-contrast T1 hyperintensity (@Key Finding 2), and enhances (@Key Finding 3), all features characteristic of a subacute infarct.The retroclival extra-axial mass with homogenous enhancement is much better seen than on non-con CT (@Key Finding 4, @Key Finding 5)! A dural tail can be seen on the sagital image extending inferiorly and on the axial image extending to the left and towards the left internal auditory canal and the mass was proven to be a meningioma. On the T2 weighted images (@Key Finding 6), the mass is seen to compress the right vertebral artery against the medulla. It likely occluded or critically narrowed the right PICA resulting in the infarct.
Brain
MRI

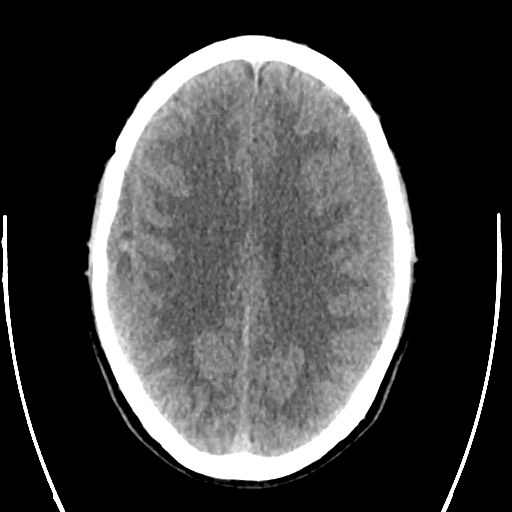
PRES (EDNeurorad Case 12a)
130 views
8 months ago
There are patchy areas of subcortical and possibly cortical hypoattenuation (@Key Finding 1, @Key Finding 2). The regions of involvement include bilateral frontal lobes, posterior parietal lobes, parieto-occipital junctions, and posterior temporal lobes. Diagnostic considerations would include multifocal areas of ischemic injury but given the posterior predominace and subcortical location, also PRES.
Head
CT
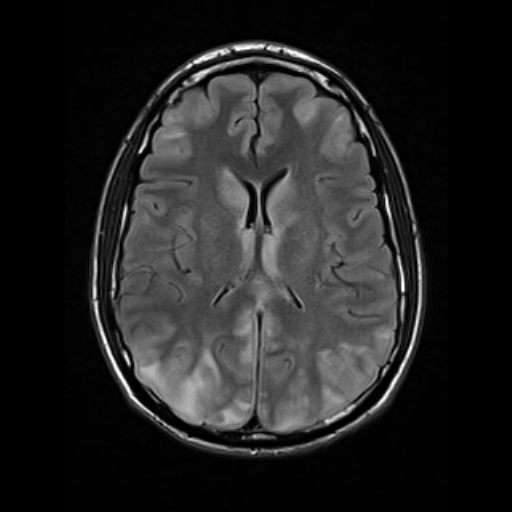
PRES (EDNeurorad Case 12b)
236 views
8 months ago
MR images more clearly depict the cortical and subcortical T2 hyperintensity with a posterior predominance (@Key Finding 1). The areas of signal abnormality demonstrated diffusion facilitation and not restriction as seen on ADC and are therefore, inconsistent with regions of acute infarction (@Key Finding 2). Note the better seen involvement of the bilateral caudate, medial thalami, and cerebella (@Key Finding 3). Patient symptoms as well as the signal abnormalities on imaging were reversible and resolved, corroborating the diagnosis of PRES.
Brain
MRI

Infarct mimic (EDNeurorad Case 13a)
113 views
8 months ago
There is loss of gray-white matter junction differentiation involving the right parietal (@Key Finding 1) and the right occipital lobe (@Key Finding 2). There is cortical swelling as evidenced by the profound effacement of the adjacent sulci compared to the left. Ordinarily, this would be consistent with a late acute infarct, however, this would require a combined right MCA and PCA territory vascular insult, which while possible, would be rare. See the followup case for further discussion.
Head
CT
Seizure related signal abnormality (EDNeurorad Case 13b)
153 views
8 months ago
The DWI and ADC images show gyriform diffusion restriction involving the right parietal and right occipital lobe (@Key Finding 1, @Key Finding 2). There is corresponding elevated FLAIR signal with cortical swelling (@Key Finding 3). Most notably, there is no elevation of TMAX (@Key Finding 4) despite the extensive region of cytotoxic edema which would be very odd for an infarct, in addition to the extensive combined MCA and PCA involvement. This patient had prolonged seizure activity accounting for these signal abnormalities. Neurological symptoms resolved after a few days corroborating the diagnosis.See: Characteristics of seizure-induced signal changes on MRI in patients with first seizures
Brain
MRI
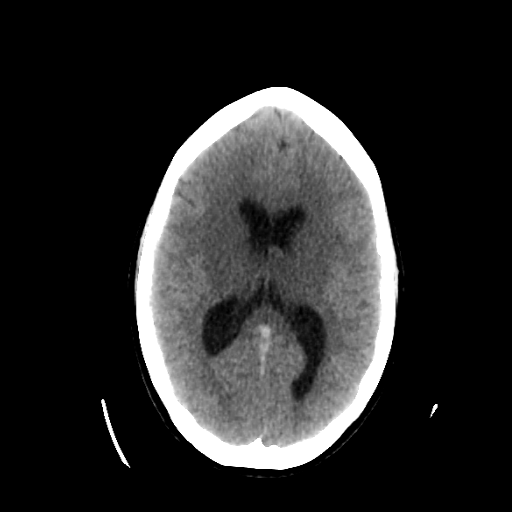
Thrombosis of straight sinus, inferior sagital sinus, vein of Galen, and internal cerebral veins (EDNeurorad Case 14a)
130 views
8 months ago
There is hypoattenuation in the bilateral basal ganglia and thalami (red outline, @Key Finding 1). While this is a finding that can be seen in hypoxic-ischemic injury, the gray-white junction differentiation elsewhere is preserved. Closer inspection reveals hyperdense appearance at the junction of straight sinus, inferior sagital sinus and the vein of Galen (red arrow, @Key Finding 1) extending to the bilateral internal cerebral veins (green arrow, @Key Finding 2). This suggests that there is venous ischemia due to dural and internal venous thrombosis.
Head
CT
Thrombosis of straight sinus, inferior sagital sinus, vein of Galen, and internal cerebral veins (EDNeurorad Case 14b)
128 views
8 months ago
CTV corroborates the presence of thrombus within the vein of Galen (green arrow @Key Finding 1) extending to both internal cerebral veins (red arrows @Key Finding 2).Sagital reformation shows nicely how the thrombus extends from the straight sinus, towards the inferior sagital sinus and into the vein of Galen (@Key Finding 3).
Head
CTA

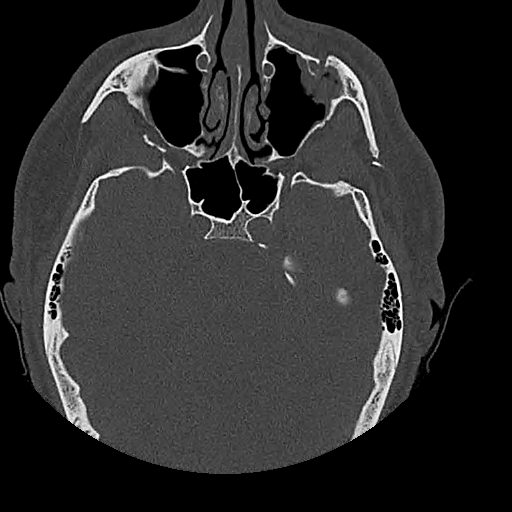
Aggressive sinusitis with intracranial extension (EDNeurorad Case 15a)
169 views
8 months ago
There is evidence of multifocal paranasal sinus inflammation with mucosal thickening. Involvement of the ethmoid sinuses is shown in @Key Finding 1. On @Key Finding 2, there is complete opacification of the left maxillary sinus but more importantly, there is stranding in the retromaxillary fat extending towards the lateral skin suggestive of aggressive sinusitis. Finally, and this is crucial to detect on imaging, @Key Finding 3 demonstrates hypoattenuation in bilateral inferior frontal lobes suggestive of intracranial extension of the infection with associated cerebritis.
Head
CT
Aggressive sinusitis with intracranial extension (EDNeurorad Case 15b)
187 views
8 months ago
MR images confirm intracranial extension of sinusitis with DWI showing restricted diffusion in the gyrus recti (@Key Finding 1) and the T1 post showing thickening of the anterior dura on both sides (@Key Finding 2).The lack of enhancement in the thickening mucosa in the left ethmoid sinuses is suggestive of devitalized mucosa (@Key Finding 3). Additionally, there are remote areas of diffusion restriction, for instance shown in the bilateral superior frontal gyri (@Key Finding 4), that represent more widespread dissemination.T2 images also show the associated soft tissue infiltration as also shown on the CT images.
Brain
MRI
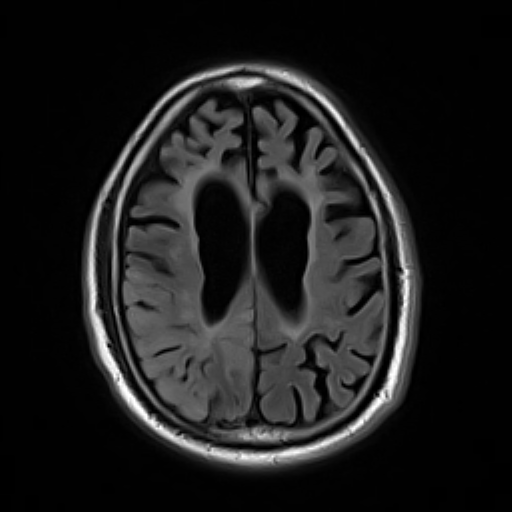
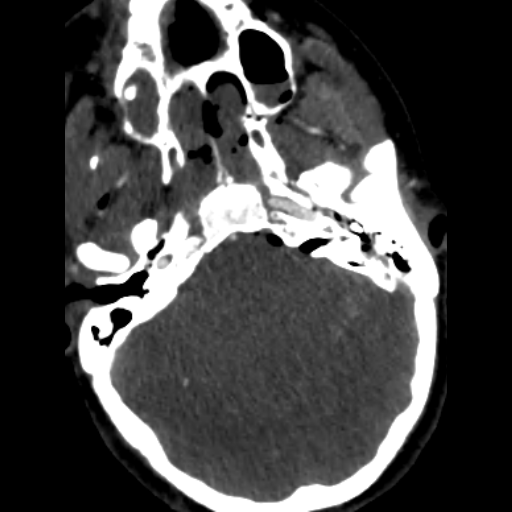
Intracranial hypotension (EDNeurorad Case 16)
159 views
8 months ago
There are bilateral low attenuation upper cerebellar convexity subdural collections (@Key Finding 1). The attenuation is slightly greater than CSF so most likely they would be chronic subdural hematomas and less likely subdural hygromas.On the axial images, near complete effacement of the prepontine cistern (shown in @Key Finding 2 as the pons flush against the clivus) can be observed. The collections above are too small to be causing this much mass effect. Looking at sagital reformations (@Key Finding 3), we can see prominent appearance of the pituitary gland, a "sagging" appearance to the brain which abuts the pituitary, as well as sagging brainstem and mild cerebellar tonsillar ectopia. These findings, in addition to the bilateral subdural collections, are quite characteristic of intracranial hypotension.
Head
CT

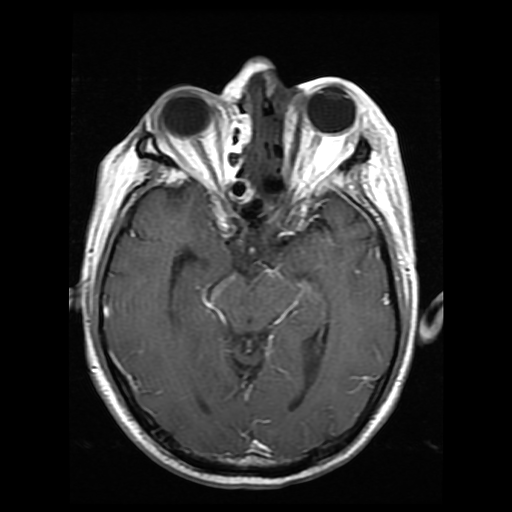
Intracranial hypotension (EDNeurorad Case 17)
136 views
8 months ago
In addition to the morphologic features of intracranial hypotension described in the precursor case (@Key Finding 1), MRI also shows characteristic diffuse pachymeningeal enhancement (@Key Finding 2). On MRI, you can also more accurately observe the ponto-mamillary distance to be small, another feature of intracranial hypotension.See: Intracranial Hypotension: Improved MRI Detection With Diagnostic Intracranial Angles
Brain
MRI
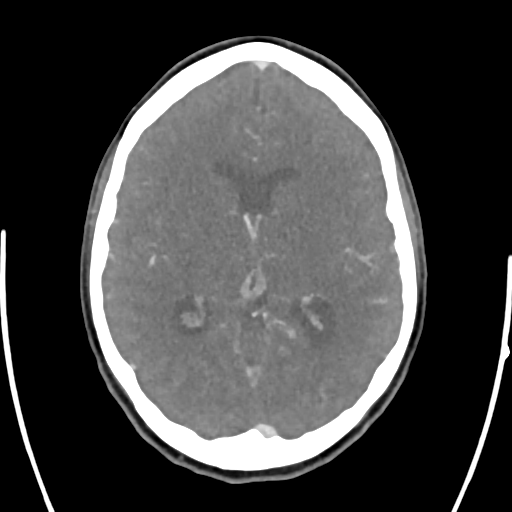
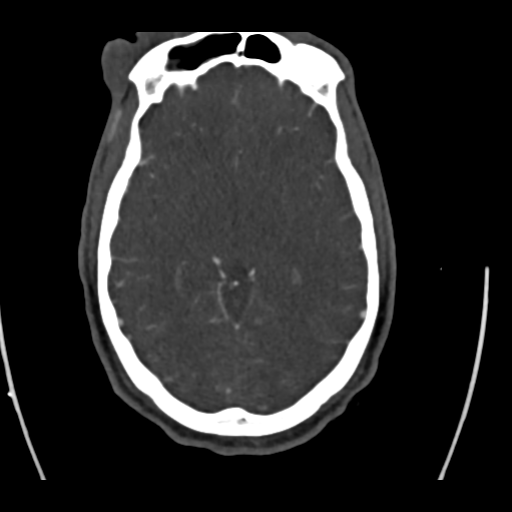
Anterior communicating aneurysm (EDNeurorad Case 18a)
139 views
8 months ago
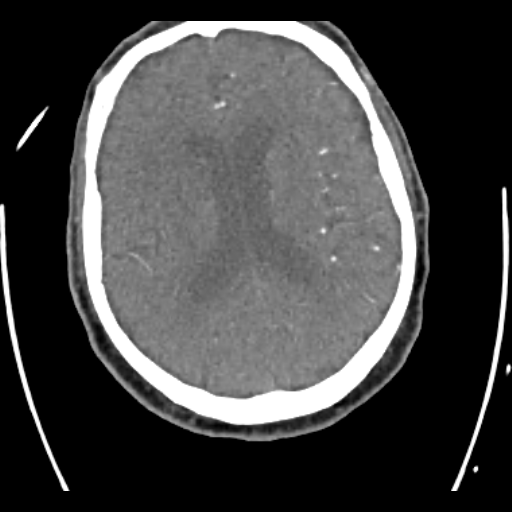
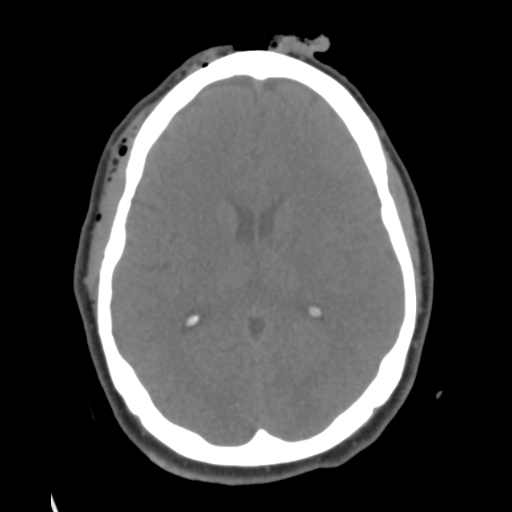
The most notable finding here is the incidental strong evidence for an anterior communicating aneurysm (@Key Finding 1, @Key Finding 2). With enough brain volume loss and with high enough resolution head CT, there is enough contrast between the arteries and the expanded CSF spaces for small aneurysms to become visible even on non-con CT.The patient does have a small right parietal scalp hematoma.
Head
CT

Anterior communicating aneurysm (EDNeurorad Case 18b)
132 views
8 months ago
CTA of course confirms the presence of a small saccular anterior communicating aneurysm (@Key Finding 1, @Key Finding 2).
Head
CTA
Left mandibular fracture (EDNeurorad Case 19)
115 views
8 months ago
The major traumatic finding here is that there is a mildly displaced, mildly angulated fracture of the left mandibular ramus at the junction with the coronoid process (@Key Finding 1). Mandibular fractures frequently "complete the ring" so we need to get whole mandible imaging to look for a second fracture given that there is no TMJ dislocation.
Head
CT

Mandibular fractures (EDNeurorad Case 20)
119 views
8 months ago
Max-face CT redemonstrates the displaced left mandibular fracture at the junction of the ramus and condylar process (@Key Finding 1). There is an additional minimally displaced right parasymphyseal fracture as well, "completing the ring." (@Key Finding 2)
Head
CT
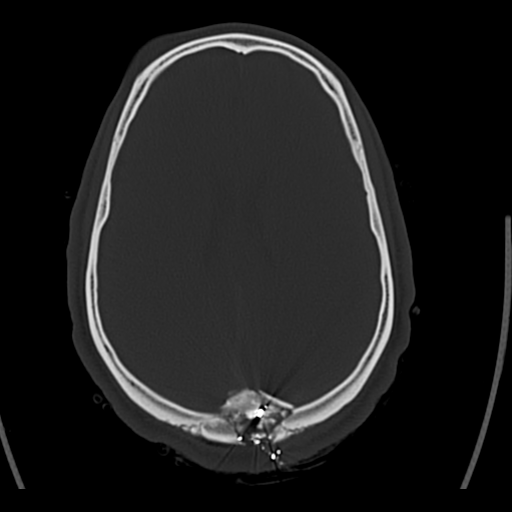
VP shunt catheter break (EDNeurorad Case 21)
136 views
8 months ago
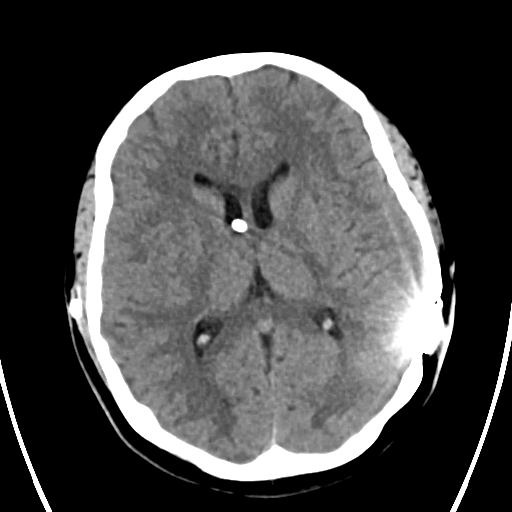
While the ventricular system is not enlarged, there is a break in the ventriculoperitoneal shunt catheter tubing inferior to reservoir, confirmed on subsequent revision (@Key Finding 1). The two ends of the broken catheter are shown in the MIP key finding image but should of course be confirmed broken by reviewing the source images as well. Always include assessment of the shunt tubing integrity part of your search pattern.
Head
CT
Left atlanto-occipital injury (EDNeurorad Case 22)
136 views
8 months ago
There is a mildly displaced fracture of the left occipital condyle (@Key Finding 1 and @Key Finding 3). In addition, there is a mildly displaced fracture of the left lateral mass of C1 (@Key Finding 2). Cervical spine CT might not always be obtained at the same time as the head CT so include the craniocervical junction in your head CT search pattern.There is also extensive soft tissue laceration to the right forehead (@Key Finding 4) with an associated minimally displaced fracture of the right superolateral orbital rim (@Key Finding 5).
Head
CT
Zygomatico-maxillary complex fracture (EDNeurorad Case 23)
140 views
8 months ago
All components of a left sided Zygomatico-maxillary complex (ZMC) fracture are present (aka tetrapod fracture): Fracture of the lateral left maxillary sinus at the level of the zygomatico-maxillary suture (@Key Finding 1), segmental fracture of the left zygomatic arch extending to the zygomatico-temporal suture (@Key Finding 2), fracture of the left zygomatico-sphenoid suture (@Key Finding 3), and fracture/diasthasis of the left zygomatico-frontal suture (@Key Finding 4).
Head
CT

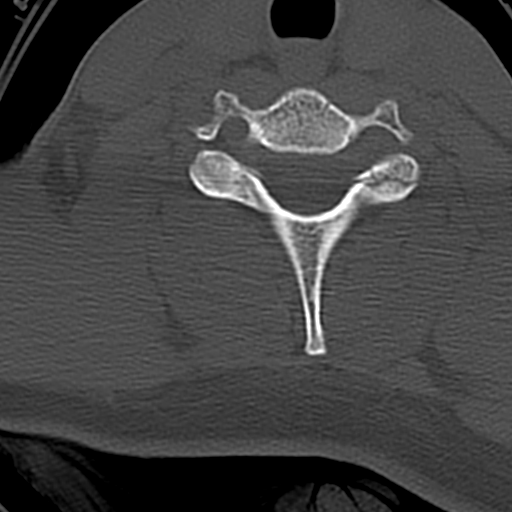
Foramen transversarium fracture (EDNeurorad Case 24)
150 views
8 months ago
There is a minimally displaced fracture of the right transverse process of C6 extending to the foramen transversarium (@Key Finding 1). The fracture line also extends to the pedicle (@Key Finding 2). When fracture lines involve the foramen transversarium, a CTA commonly follows to assess for injury to the vertebral artery.
Cervical spine
CT
Traumatic right vertebral occlusion (EDNeurorad Case 25)
134 views
8 months ago
Right foramen transversarium fracture was noted on the prior case. The most proximal portion of the right vertebral artery near its origin is noted to be patent (@Key Finding 1). There is abrupt occlusion of the vessel shortly after this point (@Key Finding 2) and the vessel remains occluded thoughout the neck. Minimal opacification is present distally from collaterals.
Head and neck
CTA

Discitis Osteomyelitis (EDNeurorad Case 26)
172 views
8 months ago
@Key Finding 1 shows typical findings of discitis-osteomyelitis: loss of disc space with associated endplate erosions and destruction. In addition, as seen in @Key Finding 2, there is substantial surrounding paraspinal soft tissue swelling (red arrow) and osseus fragments (and likely epidural extension of the infection) within the spinal canal (green arrow). MRI without and with contrast would be the modality of choice to assess for any epidural abscess.
Lumbar spine
CT

Instrumentation failure, infection (EDNeurorad Case 27)
134 views
8 months ago
The patient is status post posterior decompression with instrumentation posterior fixation spanning from the occiput to the visualized thoracic spine. The occipital plate is inferiorly displaced compared to the bone and the three midline screws have all completely backed out and are in the soft tissues (red arrows in @Key Finding 1 and @Key Finding 2).Some additional findings include lucency throughout the length of the left C1 screw consistent with infection (@Key Finding 3) as well as a fluid collection in the posterior paraspinal tissues (@Key Finding 4). Such profound lucency and instrumentation failure should be considered highly suspicious for infection.
Cervical spine
CT
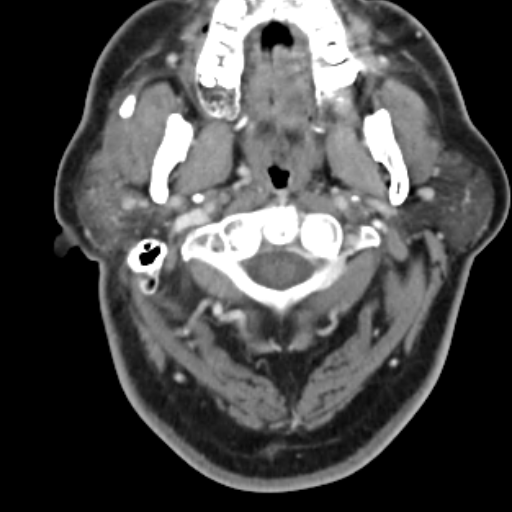
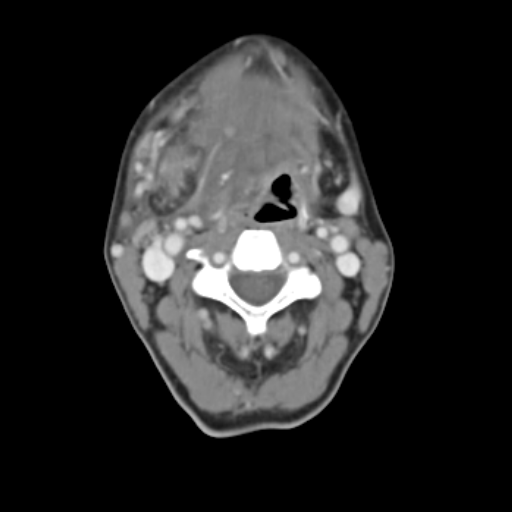
Parotiditis due to sialolithiasis (EDNeurorad Case 28)
107 views
8 months ago
There is a stone within the proximal portion of the right parotid/Stensen's duct (red arrow @Key Finding 1). There is associated dilation of the proximal duct (white arrow @Key Finding 1) and if you window just right, you can see hyperenhancement of the duct mucosa. Finally, the right parotid gland is hyperdense compared to the left due to the edema and inflammation consistent with parotiditis (green arrow @Key Finding 1).
Neck
CT
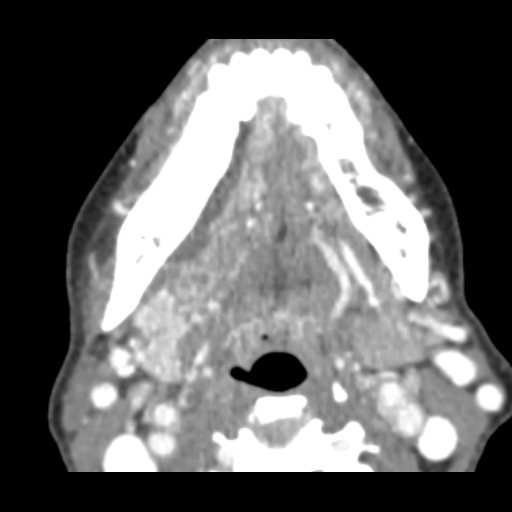
Peritonsillar abscess, palatine tonsilitis (EDNeurorad Case 29)
124 views
8 months ago
There is enlargement of both palatine tonsils with internal organized fluid collections (red arrows @Key Finding 1) consistent with palatine tonsillitis and peritonsillar abscess.
Neck
CT
Odontogenic abscess (EDNeurorad Case 30)
128 views
8 months ago
There is a right submandibular space fluid collection as shown on @Key Finding 1 and @Key Finding 2. There are numerous dental caries and periapical lucencies throughout but the first and third right mandibular molars are carious (red arrows @Key Finding 4), have periapical lucensies (green arrow @Key Finding 4), and are immediately adjacent to the fluid collection. @Key Finding 3 suggests contiguity of the fluid collection with the carious portion of the third mandibular molar. For odontogenic abscesses like this, do not rely on the presence of rim-enhancement to call an abscess. Abscesses can be small or thin and as such, not show rim enhancement. Any fluid collection next to a carious tooth with periapical lucency should be considered an odontogenic abscess until proven otherwise.
Maxillofacial
CT

Vertebral dissecting pseudoaneurysm (EDNeurorad Case 31)
111 views
8 months ago
There is a pseudoaneurysm with adjacent luminal irregularity involving the V3 segment of the right vertebral artery at the inferior C2 level (@Key Finding 1, @Key Finding 2).
Neck
CT
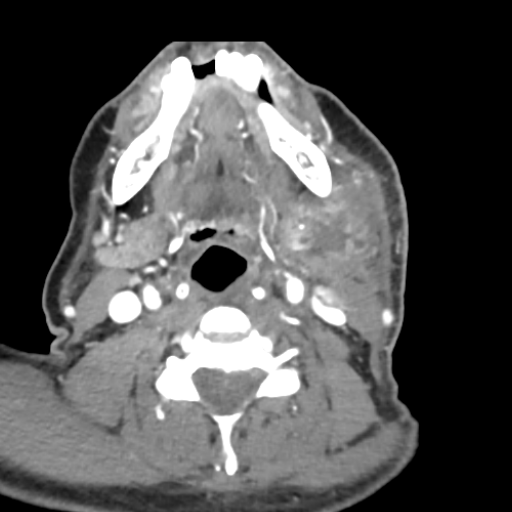
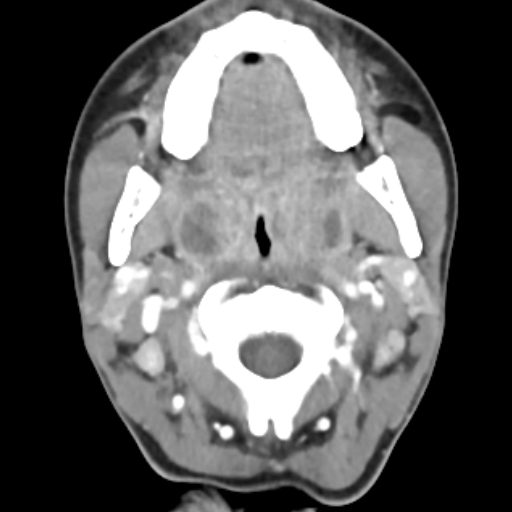
Submandibular space abscess (EDNeurorad Case 32)
107 views
8 months ago
There is a multiloculated rim enhancing fluid collection within the left submandibular space (@Key Finding 1), which combined with the substantial surrounding stranding is consistent with an abscess. While most of the left submandibular gland has a normal appearance, superiorly (@Key Finding 2) the abscess and inflammation is indistinct from the gland and potentially arising focally from the gland. There is no sialolithiasis. There is additional thickening and asymmetric enhancement in the left oropharynx and palatine tonsil (@Key Finding 3), likely reactive as the epicenter of the major inflammation is clearly in the submandibular space.
Neck
CT
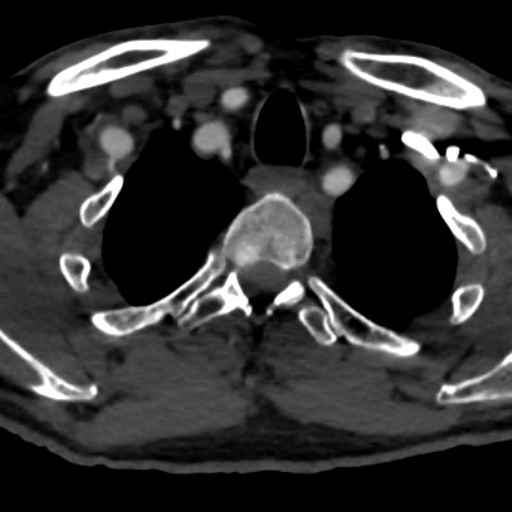
Right face cellulitis, metastatic papillary thyroid cancer, pulmonary adenocarcinoma (EDNeurorad Case 33)
130 views
8 months ago
@Key Finding 1 demonstrated right facial cutaneous thickening (white arrow) with subcutaneous stranding and thickening of the platysma muscle (red arrow) which are suggestive of underlying cellulitis. The source of the infection is not clear. There is clearly lymphadenopathy in the right neck. While in the setting of cellulitis having reactive lymphadenopathy is quite common, close inspection reveal a punctate peripheral calcification associated with one of the nodes (green arrow in @Key Finding 1). Such calcifications should raise the suspicion for metastatic papillary thyroid cancer.The coronal image (@Key Finding 3) shows the elongated appearance of the right upper pole of the thyroid and the axial image shows a punctate calcification within this elongated region (@Key Finding 2). By imaging, this is extremely suspicious for underlying papillary thyroid cancer and metastatic lymphadenopathy, which were pathologically confirmed.But there's more to this case! Inspection of the lungs reveals pulmonary nodules (@Key Finding 4), both solid (for instance in the right upper lobe) and subsolid/groundglass (as seen in the left upper lobe). While the solid nodules would be suspicious for metastatic disease, the ground glass nodule is atypical. These were biopsied and proven to be pulmonary adenocarcinoma.
Neck
CT
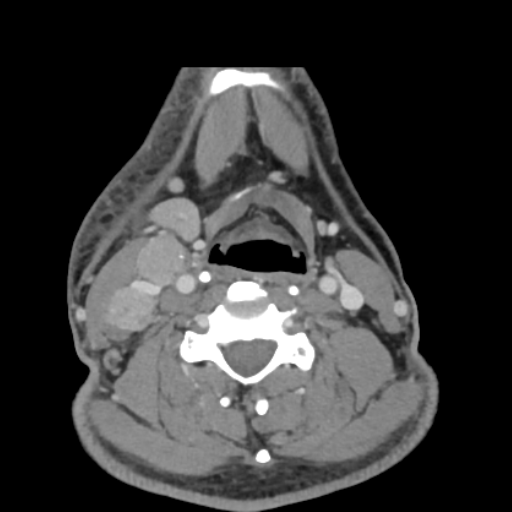
Submandibular sialadenitis due to sialolithiasis (EDNeurorad Case 34)
116 views
8 months ago
Due to underlying Sjogren's syndrome, there is extreme fatty replacement of both submandibular (shown on @Key Finding 1) and the parotid glands. However, the right submandibular gland is enlarged compared to the left, has internal edema and increased attenuation, substantial surrounding stranding as well as infiltrative edema extending to the adjacent tissues. Notice how on @Key Finding 1, the edema extends to the right aspect of the oropharynx and results in effacement of the right vallecula compared to the left (green arrow).On @Key Finding 2, you can see bilateral distal submandibular duct stones. There are quite a few more stones (@Key Finding 3, @Key Finding 4). The right submandibular duct is dilated (@Key Finding 4 and @Key Finding 5) and has mucosal hyperenhancement (@Key Finding 5).These constellation of finding are consistent with right submandibular sialadenitis due to sialolithiasis.
Neck
CT
Bilateral facet fractures (EDNeurorad Case 35)
108 views
8 months ago
There is a comminuted fracture of the left C7 superior articular process with intra-articular extension to the C6-C7 facet joint (@Key Finding 1 and @Key Finding 2).An additional minimally displaced fracture is also present on the right involving the tip of the superior articular process as best shown on sagittal images (@Key Finding 3 and @Key Finding 4).Finally, a very subtle non-displaced fracture of the C6 posterior spinous process (@Key Finding 5 and @Key Finding 6)
Cervical spine
CT
Communited gunshot fracture, subdural hematomas, concern for superior sagittal sinus injury (EDNeurorad Case 36)
100 views
8 months ago
There is a comminuted and depressed gunshot fracture centered in the inferior part of the sagittal suture with fracture lines in both parietal bones as well as in the upper part of the occipital bone. The fracture lines also involve the upper part of the sigmoid sutures (red arrows in @Key Finding 1).The immediate vicinity of the gunshot fracture is suboptimally assessed due to the streak artifact. But scrolling above the gunshot fragments, and using subdural windows, there are bilateral extra-axial hemorrhages (red arrows in @Key Finding 2 and @Key Finding 3) likely subdural in location.One important point is that the location of the gunshot injury and depressed fracture fragments at the sagittal suture should raise concern for injury to the superior sagittal sinus. Therefore, a CTV is likely prudent as a next imaging step.
Head
CT
Traumatic superior sagittal sinus thrombosis (EDNeurorad Case 37)
126 views
8 months ago
CTV images show that the posterior half of the superior sagittal sinus is occluded consistent with traumatic thrombosis. @Key Finding 1 shows that the occlusion extends further inferior to the epicenter of the gunshot fracture. @Key Finding 2 shows the approximate upper and lower margins of the thrombosis (red arrows)
Head
CTA

Maxillary alveolus fracture (EDNeurorad Case 38)
110 views
8 months ago
There is a minimally displaced fracture of the left maxillary alveolus involving the socket to the left medial incisor tooth (@Key Finding 1 and @Key Finding 2). These fractures are easily missed on imaging. Clinically they are more apparent because the involved tooth is often loose and may be bleeding.
Head
CT

Complex lumbar spine fractures, suspected posterior ligamentous complex injury (EDNeurorad Case 39)
145 views
8 months ago
Clearly there are compression fractures of the L2 and L3 superior endplates (@Key Finding 1). The sclerotic lines in the upper portion of the vertebral bodies are due to compressed bone. The upper part of the posterior cortices is also buckled to the spinal canal. If you want to use the Thoraco-Lumbar Injury Classification and Severity (TLICS) terminology, you may call the morphology of this fracture as "burst" but there are more findings to consider. In particular, the interspinous distance at L1-L2 appears increased compared to the remaining interspinous distances, a finding that should raise suspicious (but is not definitive for) injury to the posterior ligamentous complex.@Key Finding 2 (Sagittal image through patient's right) shows a horizontally oriented fracture through the posterior elements at L2 on the right side. @Key Finding 3 on the other hand shows fractures of the left superior articular process of L2 with mild widening of the left L1-L2 facet joint compared to the right. Based on these additional fracture, one can make the case that the fracture is best described as a distraction pattern or "Chance" fracture. Regardless, these additional fractures make an injury to the posterior ligamentous complex much more likely and so an MRI is warranted to assess the ligaments.The L2 left transverse process is also fractured but it's not of much concern!
Lumbar spine
CT

Lumbar fractures with posterior ligamentous complex injury (EDNeurorad Case 40)
131 views
8 months ago
Sagittal STIR images show the marrow edema associated with the fractures with saw on CT. There is clearly edema within the interspinous space at L1-L2 (@Key Finding 1) consistent with injury to the interspinous ligament. On the left, there is focal disruption of the ligamentum flavum at the L1-L2 level consistent with traumatic injury/rupture (@Key Finding 2). On the right, the curvilinear STIR hyperintensity is likely within the bone and corresponds to the fracture line we saw on the prior CT (@Key Finding 3).One final finding in this case is the prominence of the posterior epidural fat as seen on sagittal T1 images (red arrows @Key Finding 4) which when correlated with the STIR image, demonstrates superimposed edema. The result is severe crowding in the thecal sack as can be seen on the axial images (orange arrow @Key Finding 5)
Lumbar spine
MRI
Complex trauma (EDNeurorad Case 41)
138 views
8 months ago
This is a busy case with many findings. I always start with the brain and intracranial findings before getting bogged down on all the fractures. There are multifocal areas of parenchymal hemorrhage (@Key Finding 1) with hemorrhages in the left frontal lobe inferiorly annotated on the above panel. Additional multifocal subarachnoid hemorrhages are also present (blue arrows) shown in particular in the medial left middle cranial fossa (@Key Finding 23), the left sylvian fissure @Key Finding 24, the left frontal lobe @Key Finding 25, and the left upper cervical spine @Key Finding 26. Finally, there is subdural blood and gas in the left temporo-occipital junction convexity (green arrow @Key Finding 27).Additional findings are the presence of subarachnoid gas in the basilar cisterns as well as diffuse effacement of the sulci and particularly the basilar cisterns suspicious for cerebral edema. Now on to the fractures!Knowing the basic fracture patterns can be helpful in cases like this, more than anything to know what fractures tend to occur together and to be more concise in our impressions.The components of a naso-orbito-ethmoid (NOE) fracture pattern are present including fracture of the nasal bone (right sided, shown on axial @Key Finding 2), medial orbital walls @Key Finding 4, adjacent ethmoid sinuses (@Key Finding 4 the exact fractures are difficult to see but the substantial opacification implies fractures), and the nasal septum (seen best on the coronal plane, both anteriorly @Key Finding 3 and posteriorly @Key Finding 5).On the left, there are fractures of the pterygoid plates (red arrow on axials @Key Finding 6). Whenever, you see pterygoid plate fractures, look for the other component of LeFort fracture patterns. On the coronal images, a horizontal fracture of the left anterolateral nasal aperture with associated horizontal fracture of the left lateral maxillary sinus wall are present completing a LeFort I pattern (red arrows @Key Finding 7).There is fracture of the anteromedial orbital wall, the inferior orbital rim and floor, which combined with the nasal bone and lateral maxillary sinus wall fractures form the components of a LeFort II pattern @Key Finding 8. However, I do not think that the nasal bone fracture @Key Finding 9 has the characteristic transverse orientation you're supposed to have for a LeFort II and it seems separate and not extending to the medial orbital wall fracture. Therefore, I would just describe the components here and not specifically mention that there is a LeFort II fracture (this study was however read as having a LeFort II fracture so not everyone always agrees).There is no lateral orbital rim or zygomatic arch fractures on the left so no LeFort III. No pterygoid plate fracture on the right means no LeFort fracture on that side.The components of a ZMC fracture are present on the right: fracture of the zygomatic arch and mild diasthasis at the zygomatico-temporal suture (@Key Finding 10 and @Key Finding 11), comminuted fracture of the antero-medial maxillary sinus walls near the zygomatico-maxillary suture (@Key Finding 12), fracture of the zygomatico-sphenoid suture (@Key Finding 13), and fracture at the level of the zygomatico-frontal suture (@Key Finding 14).Once I've done a pattern based search for the fractures, I then go through the paranasal sinuses, nasal cavity, orbits, and skull base and see what's fractured.In the paranasal sinuses, there is fracture of the right frontal sinus inner wall with intracranial extension (@Key Finding 15). All the walls of the sphenoid sinuses and the sphenoid septum have been fractured (@Key Finding 16). A fracture fragment protrudes to the right superior orbital fissure (rightmost blue arrow in @Key Finding 16).When looking at the sphenoid and ethmoid sinuses, it's important to look at the roofs, best seen on coronal and sagittal planes. Here, the ethmoid roof and the planum sphenoidale are fractured, predisposing the patient to CSF leakage (@Key Finding 17).All the walls of the maxillary sinuses are fractured (green arrows @Key Finding 18), some of which we have already discussed as part of the fracture patterns.In the orbits, on the right, all the walls are fractured (@Key Finding 19), including the roof with intracranial extension and pneumocephalus. The orbital floor fracture is comminuted and highly depressed. On soft tissue recons, there is herniation of orbital fat and inferior rectus muscle through the fracture defect (@Key Finding 20). The inferior rectus muscle is thickened compared to the contralateral side consistent with intramuscular hematoma. Clinical assessment for the presence of entrapment is likely prudent. Also mention how much orbital hemorrhage there is, here mainly extra-conal and in the supero-lateral orbit (green arrow @Key Finding 20).On the left, there is also a fracture of the roof. The medial and floor fractures we have already described. There is not much displacement of the fractures and not as much intra-orbital hemorrhage.The globes should be assessed and here there is no evidence of injury. There is of course peri-orbital soft tissue swelling and gas.Finally, looking at the remaining skull base/calvarium, one sees that the right sphenoid sinus fractures have a component extending along the greater wing of the right sphenoid (red arrow @Key Finding 21).In the nasal cavity, there is a fracture of the right hard palate (blue arrow @Key Finding 22). This and palate fractures in general are also very well seen on coronal reformations.Interrogating the mastoids and middle ears, there is most likely a left mastoid fracture given the large effusion in the mastoids and middle ear (green arrow @Key Finding 22). However, the fracture line is not evident on these images.
Head
CT
Right carotid traumatic injury (EDNeurorad Case 42)
112 views
8 months ago
This is a followup of EDNeuroRad Case 41. See the prior case for discussion of additional extensive traumatic findings.Inferior to the skull base, there is an intimo-medial flap in the right internal carotid artery which extends to the junction of the cervical and petrous segments (@Key Finding 1). There is near occlusion of the vessel prior to skull base entry (@Key Finding 2). Further superiorly, there is an area of what appears to be moderate to severe narrowing of the right ICA in the distal cavernous segment immediately adjacent to the anterior clinoid process, suspicious for an additional site of injury (@Key Finding 3).
Neck
CT